|
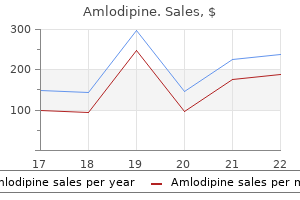
Amlodipine dosages: 10 mg, 5 mg, 2.5 mg
Amlodipine packs: 30 pills, 60 pills, 90 pills, 120 pills, 180 pills, 270 pills, 360 pills

10 mg amlodipine cheap visaThe fibrous variant of Hashimoto thyroiditis has important deposition of dense fibrous tissue with effacement of the thyroid architecture and follicular atrophy blood pressure chart example cheap amlodipine 2.5 mg overnight delivery. However arrhythmia 101 buy amlodipine 2.5 mg online, not like invasive fibrous thyroiditis arrhythmia reference guide amlodipine 5 mg order with amex, the method is restricted to the thyroid gland hypertension updates generic amlodipine 5 mg otc, and oncocytic metaplasia is characteristically current. The diffuse sclerosing variant of papillary carcinoma demonstrates quite a few psammoma our bodies, lymphocytic thyroiditis, and areas of tumor with the diagnostic nuclear features of papillary carcinoma. The chief morbidity is said to hypothyroidism, since the native effects of the goiter may be addressed surgically, if needed. Other potential complications include hypoparathyroidism and nerve injury related both to the illness or to the difficulty of surgical procedure in these patients. In those people with multifocal systemic fibrosclerosis, different organ techniques may be affected by life-threatening illness. Corticosteroid remedy has been profitable within the majority of patients in controlling disease development or in full or partial reversal of symptoms. A fibrous variant is related to marked fibrosclerosis and atrophy of the thyroid epithelium. A combination of genetic and environmental components (the latter including high iodine intake, infections, drugs, being pregnant, and smoking) probably play a job and in the end result in a breakdown of immune tolerance. The activated helper T-cells, in flip, stimulate autoreactive B-cells to be recruited into the thyroid, where they secrete autoantibodies. Symptoms of hypothyroidism embody constipation, pores and skin adjustments, bradycardia, menstrual cycle abnormalities, melancholy, and myxedema. Severe hypothyroidism is usually related to the fibrous variant of the illness. Rare sufferers current with hyperrather than hypothyroidism, known as hashitoxicosis. Juvenile Hashimoto thyroiditis, often seen in adolescents and younger adults, may current with hypothyroidism or hyperthyroidism; the patients usually have a powerful household history of thyroid disease. Some patients also have hypoadrenalism (Schmidt syndrome), hypoparathyroidism, diabetes mellitus, or hypogonadism. An exception to that is the fibrous variant of Hashimoto thyroiditis, which is more common in older males. The danger of the illness appears highest in nations with the very best iodine consumption (United States and Japan). Other autoimmune illnesses could coexist, together with pernicious anemia, sort 1 diabetes mellitus, a quantity of sclerosis, rheumatoid arthritis, Addison illness, Graves disease, and Sj�gren syndrome. Patients with persistent lymphocytic thyroiditis have a gradual, diffuse enlargement of a firm, nontender thyroid gland, usually 2 to 3 occasions the traditional weight. Ultrasound characteristically shows heterogeneous parenchyma with innumerable small hypoechoic nodules separated by echogenic septae. Radioactive iodine uptake is usually regular or increased in Hashimoto thyroiditis, suggesting Graves disease, even in patients with hypothyroidism. If the illness is of lengthy standing, it may comprise distinct nodules and bands of fibrous tissue. The fibrous variant could be very firm and fibrotic, with a multinodular minimize floor resembling cirrhosis of the liver. The thyroid gland could additionally be fairly small (< 5 g) within the late stage ("fibrous atrophy variant"). B, the reduce floor of lymphocytic thyroiditis bears a hanging resemblance to lymph node tissue. The lymphocytic infiltrate is normally confined to the thyroid however rarely extends into the adjacent delicate tissue. The appearance of the follicular epithelium may range from area to area, with some follicles remaining intact. The oncocytic (H�rthle) cells are strikingly totally different from regular follicular epithelial cells. The cytoplasm of the oxyphilic cells is ample, eosinophilic, and really granular. Squamous metaplasia is common in the atrophic follicular epithelium, significantly in more superior circumstances and in the fibrous variant. The juvenile type has the lymphocytic infiltrate but tends to include minimal follicular atrophy and oncocytic metaplasia. The fibrous variant of Hashimoto thyroiditis, also referred to as "advanced lymphocytic thyroiditis," represents ~10% of cases. A lobular pattern continues to be evident from the distribution of the lymphoid infiltrate around the severely atrophic follicles. The atrophic variant ("fibrous atrophy") has more excessive follicular atrophy and sure represents end-stage illness. If lymphoma is suspected, it could be prudent to reserve fresh tissue in transportation media for move cytometric immunophenotyping. The plasma cells in the background are polyclonal for immunoglobulin heavy and light chains. Whether or not these circumstances fall within the spectrum of IgG4-related illness is controversial. The follicular epithelium is usually scant, present in small flat sheets or as single cells. The nuclei of the epithelial cells could additionally be enlarged; they might embody vesicular or "pale" chromatin and irregular nuclear contours. Cellular adenomatoid nodules may be indistinguishable from a follicular neoplasm by cytology alone; examination of the periphery of the nodule histologically is important to make that distinction. Rapid enlargement of the gland, a diffuse, sheet-like effacement of the thyroid parenchyma, lymphoepithelial lesions, and supporting immunohistochemistry and/or circulate cytometry will help to make the diagnosis of lymphoma. They are often seen as small sheets of polygonal cells with ample granular blue cytoplasm. B, A nice needle aspiration yields a dense infiltrate with a polymorphous lymphoplasmacytic population with oncocytic follicular epithelium showing orangeophilic (alcohol-fixed, Papanicolaou stain). Invasive fibrous thyroiditis has a diffuse pattern of effacement by fibrosis that infiltrates beyond the thyroid gland and is accompanied by vasculitis. It is incessantly encountered as an incidental discovering in thyroids resected for other causes and not accompanied by oncocytic metaplasia. Painless or silent thyroiditis (sporadic or postpartum) is considered by some to be a variant of chronic lymphocytic thyroiditis. It is characterized by transient hyperthyroidism followed by hypothyroidism that ultimately resolves in most cases. However, thyroid glands usually include a lymphoplasmacytic infiltrate with out vital oncocytic metaplasia. Surgery could also be really helpful if the thyroid enlargement is symptomatic or if suspicious nodules develop. The increased incidence of lymphoma, normally an extranodal marginal zone B-cell lymphoma (although transformation to a diffuse large B-cell lymphoma additionally occurs) suggests lifelong monitoring to exclude this growth. The immune abnormality is mediated by antibodies to the thyrotropin receptor discovered on follicular epithelial cells. The clinical effect of this autoimmune course of is thyrotoxicosis (hyperthyroidism), accompanied by diffuse thyroid enlargement, an infiltrative ophthalmopathy in about 25% of sufferers, and a spectrum of systemic effects of thyroid hormone extra. The incidence is approximately 1% to 2% of the inhabitants, with a slightly greater incidence in areas of notably high iodine intake (United States and Japan). Men, however, are probably to develop Graves illness at an older age, often with a extra extreme type of thyrotoxicosis. The signs of Graves illness replicate the effect of thyrotoxicosis and of the autoimmune process on multiple organ methods. The spectrum of indicators and signs contains weight reduction, heat intolerance, fatigue, weak point, palpitations, dyspnea on exertion, stridor as a result of tracheal compression, hoarseness, chest pain, dysphagia, oligomenorrhea, hair loss or change in hair texture, a "gritty" sensation within the eyes, proptosis, conjunctivitis, memory loss, poor attention span, emotional lability, muscle weakness, and irritability or agitation. In addition, the thyroid is diffusely enlarged and a bruit may be appreciated over the thyroid space. Also, long-standing or handled Graves illness is usually characterised by the event of nodules.
Diseases - Arthrogryposis ectodermal dysplasia other anomalies
- Rhizomelic dysplasia type Patterson Lowry
- Chromosome 12p deletion
- Hypogonadism mitral valve prolapse mental retardation
- Sosby syndrome
- Placenta disorder
Amlodipine 5 mg buy mastercardSites outdoors the top and neck embody the mediastinum heart attack unnoticed cheap amlodipine 10 mg otc, stomach blood pressure pregnancy range amlodipine 2.5 mg buy free shipping, prostate gland blood pressure and anxiety order amlodipine 10 mg fast delivery, rectum blood pressure j curve amlodipine 10 mg cheap with visa, and vulva. Removal of these salivary gland tissue deposits may happen for beauty causes, as intervention for a congenital abnormality (oncocytosis), or due to neoplasia. In the case of malignancy, confusion might come up, significantly if the remaining normal gland architecture has been destroyed, as to whether or not the tumor is main in heterotopic salivary gland tissue versus a metastatic deposit from a nearby salivary gland. In contrast, accessory salivary glands are defined as isolated lobules of glands situated along a major salivary duct. Heterotopic or ectopic salivary gland tissue has been reported in a myriad of anatomic places (Table eleven. Oncocytes are characterized by the presence of plentiful finely granular, shiny eosinophilic cytoplasm surrounding a spherical nucleus that incorporates a single nucleolus. The quantity and distribution of oncocytic cells in salivary gland vary, as does the expansion sample. The prevalence of oncocytic cells in salivary gland could be categorized as oncocytic metaplasia within a duct or isolated aggregate, focal and diffuse oncocytosis, multifocal oncocytic hyperplasia, and oncocytoma. Oncocytic metaplasia involves the irregular change or transformation (metaplasia) of acinar cells (serous, mucous, and seromucous) and/or striated ducts to oncocytes. Oncocytic metaplasia is unusual before the age of 50 and will increase with advancing age. The metaplasia is often seen focally within a duct and may be found at the aspect of salivary gland neoplasms (pleomorphic adenoma, mucoepidermoid carcinoma). Oncocytosis is an unencapsulated (mass-forming) collection of oncocytes, which may occur in minor or major salivary glands. This alteration may contain either ducts, predominantly, or acini and could additionally be related to fatty infiltration and acinar atrophy. These nodules or islands could also be massive, however they lack the encapsulation of an oncocytoma. It is value highlighting that these oncocytic islands throughout the lymph nodes may be incorrectly confused with metastatic deposits. Histologic examination of an oncocytic lesion exhibits the characteristic polygonal cells with ample finely granular eosinophilic cytoplasm. The nuclei are often uniformly spherical with granular chromatin and comprise a single nucleolus. There may be unencapsulated focal cystic areas with papillary proliferations within ducts or as an isolated parenchymal aggregate. The nodular proliferations are seen diffusely throughout the parotid gland tissue. On ultrastructural evaluation, abundant mitochondria might utterly fill the cytoplasmic compartment. The mitochondria show some variability in their shape, starting from spherical to irregular and elongate. On fine needle aspiration, oncocytes are simply identified with plentiful, well-defined, finely granular cytoplasm and enormous round nuclei with outstanding nucleoli. However, distinguishing oncocytic metaplasia from oncocytomas is done on excised lesions. Heterotopias are excised for symptomatic reduction in some instances, with a superb prognosis. Some authorities outline an oncocytoma as a single nodule, whereas others require the presence of at least a partial capsule. The distinction between oncocytic hyperplasia and neoplasia is still not well outlined. Oncocytic metaplasia and a wide range of clear cell neoplasms are included within the differential prognosis with oncocytoma. Areas of oncocytic metaplasia have been reported in pleomorphic adenomas and inside mucoepidermoid carcinomas; nevertheless, these areas are usually isolated. The mucus retention cyst is more widespread in the parotid and submandibular glands, and the peak incidence is in the 7th to eighth decade. The extravasated type is the most typical mucocele, and its peak incidence is in the third decade. The extravasated sort mostly occurs in the lower lip, typically showing as blue-tinged, dome-shaped swellings. A large mucocele that may come up within the floor of the mouth from the sublingual or minor salivary gland and descend into the soft tissues of the floor of the mouth known as a ranula. A sialolith is a group of typically laminated concretions that kind a stone throughout the salivary gland excretory duct system. The stone will trigger distention of the duct system and retention of secreted fluids, leading to glandular swelling and ache. As the lesion progresses, granulation tissue from the wall turns into extra outstanding and organizes to obliterate the lumen of the mucocele. Lithotripsy, sialoendoscopy, and different supportive measures are used for symptomatic sialoliths. Certainly, a resolving extravasated mucocele with only remaining granulation tissue could also be misinterpreted as a small hematoma or a thrombus. However, the usage of mucicarmine would illustrate the presence of mucin-laden macrophages and aid in this distinction. The mucus retention cyst is lined by a thin layer of cuboidal epithelium with little to no inflammatory cell infiltrate. Mucoepidermoid carcinoma could enter the differential diagnosis of a mucus retention cyst. However, mucoepidermoid carcinoma incorporates three cell varieties: mucus goblet cells, intermediate cells, and squamous cells. Moreover, within mucus retention cysts, the epithelium is attenuated and it lacks papillary projections that often protrude into the lumen of a mucoepidermoid carcinoma. The clinical and histologic traits resemble those of malignant neoplasms and can lead to misdiagnosis and inappropriate remedy. Duration of healing of this lesion can vary up to 6 months, although most heal within 1 month. Other symptoms related to this lesion (pain or numbness) could simulate malignancy. Lesions are most commonly unilateral; however, occasional bilateral or midline lesions develop. Other frequent websites for this lesion are oral cavity, lower lip, retromolar trigone, tongue, and buccal mucosa, though the whole higher aerodigestive tract could be affected. Occurrence of this lesion in main salivary glands, primarily the parotid gland, is unusual, representing eight. The chief differential diagnoses for this lesion are mucosal squamous cell carcinoma and mucoepidermoid carcinoma. In addition, the inflammatory infiltrate characterizing necrotizing sialometaplasia is more prominent than that incessantly associated with squamous cell carcinoma and mucoepidermoid carcinoma. This lesion may occur in youngsters and adults of both sex; nevertheless, most instances current in women within the 4th and 5th decade. Patients experience facial swelling with or without pain, dry mouth, and keratoconjunctivitis. The changes in minor glands include a continual lymphocytic sialadenitis usually without epithelial hyperplasia. Numeric grading techniques are used based on the variety of lymphocytic aggregates present in salivary gland lobules, however clinical and serologic confirmation is required for a definitive prognosis. An mixture (50 lymphocytes) is referred to as a "focus," resulting in a "focus score. Fresh tissue at the time of biopsy could additionally be submitted for flow cytometry evaluation and gene rearrangement studies to exclude a lymphoma. The gross appearance could be mistaken for a neoplastic course of because of the multinodularity; nonetheless, the capsule in main salivary glands is undamaged. The remaining excretory ducts are usually infiltrated by intermediate-sized lymphocytes.
Discount amlodipine 5 mg on lineHowever blood pressure medication enalapril amlodipine 5 mg cheap, with a constellation of architectural and cytomorphologic features cardiac arrhythmia chapter 11 purchase amlodipine 5 mg visa, accurate prognosis of papillary carcinoma is achievable blood pressure medication iv amlodipine 2.5 mg trusted. Even though rare in kids blood pressure grapefruit 5 mg amlodipine buy with visa, papillary carcinoma continues to be the most common pediatric thyroid malignancy. Dysphagia, stridor, and cough are normally seen in patients with massive tumors as a result of compression. There are many "incidental" papillary carcinomas (discussed later), that are regularly found during routine radiographic studies for unrelated causes or in patients with other thyroid illnesses. However, serum thyroglobulin levels can be used to monitor disease status (if elevated). Ranging from microscopic to 20 cm, infiltration into the surrounding thyroid parenchyma is incessantly famous, along with extension beyond the thyroid gland periphery. Gritty, dystrophic calcification is frequent, while cystic change and hemorrhage may also be current. The best sections to submit seize the "tumor-to-capsule-to-parenchyma" interface. The prognosis of papillary carcinoma is made by using an aggregate of architectural and cytologic options, with nobody single feature being diagnostic. The precise variety of features needed for the analysis is undefined, however the nuclear features have to be current to be diagnostic. Only macroscopic evidence of extrathyroidal extension, nonetheless, is evaluated in staging. If a single tumor has many different development patterns, suspicion for papillary carcinoma should be raised. The cytomorphologic and nuclear options are vital within the diagnosis of papillary carcinoma and are normally fixed even between the variants. These options are greatest assessed on the periphery of the tumor, where comparability can be made to the adjoining, uninvolved regular thyroid tissue. There is welldeveloped nuclear chromatin clearing (optical clearing: Orphan Annie nuclei). If slides are left on the heating block for too lengthy or in an aqueous solution during processing, "false" intranuclear bubbles are created. Nuclear envelope irregularities are harder to assess on frozen part materials. The cytoplasm is variable and normally not helpful in the analysis, although variants are named in accordance with the cytoplasm (clear, oncocytic, hobnail, columnar). Likewise, their presence in lymph nodes is pathognomonic for metastatic illness (any papillary sample tumor may cause psammoma bodies), although potentially excluded in staging systems. Intratumoral fibrosis is an acellular, sclerotic, dense, eosinophilic fibrosis present in up to 90% of instances. An initial pass using a 25-gauge needle-without suction- yields excellent materials uncontaminated by blood. The nuclei are enlarged and overlapped with irregular borders, however with a powdery/dusty, delicate nuclear chromatin on alcohol mounted preparations. Colloid is often scant and thickened ("chewing gum" or ropy), with occasional multinucleate giant cells and, hardly ever, psammoma our bodies. The features of papillary carcinoma are best appreciated with alcohol-preserved Papanicolaou preparations rather than with air-dried material. With noninvasive follicular pattern tumors now recognized separately, they may present the nuclear options of papillary carcinoma. Note the variable membrane and cytoplasmic expression in the tumor cells (heavy in A), together with an space of invasion (B). Each mutation/fusion/rearrangement has distinct phenotypic and biologic properties. It is value noting that noninvasive follicular thyroid neoplasm with papillary-like nuclear features is included within the differential prognosis of follicular patterned tumors, and shall be further discussed within the chapter on benign neoplasms. However, the prognosis is great, with greater than 90% 20-year survival fee and a lower than zero. There are differences in structure and cytology, even at this low magnification. However, this represented metastatic disease from an ipsilateral main papillary carcinoma. Age (<55 years) and sex (female) are crucial prognostic components, though tumor size (> four cm), gross extrathyroidal extension, and metastasis are significant for patients fifty five years. Surgery is the remedy of choice, though the extent of surgical procedure (lobectomy, subtotal, or complete thyroidectomy) stays controversial. Recurrent laryngeal nerve damage and hypoparathyroidism are recognized surgical complications. However, the tumor must show uptake of the radiolabeled iodine to be therapeutically sensitive. The encapsulated with invasion sort shows either capsular or lymphovascular invasion. In these cases, "encapsulated variant with invasion" is used to qualify the sort of invasion. Inset demonstrates an area of increased cellularity and the cytologic features of papillary carcinoma. Nuclear grooves, nuclear contour irregularities, and nuclear chromatin clearing is accentuated. This variant appears to metastasize much less regularly than traditional papillary carcinoma, but in any other case is similar in remedy and consequence. Some authors use a lower cutoff, but this tends to dilute the category, with a couple of even suggesting a follicular oncocytic variant. The oncocytic cytoplasm is compact and "glassy" with a fine granularity, representing an increased number of mitochondria. Oncocytic cells could be seen in the tall cell variant of papillary carcinoma, from which it should be separated. Occasionally, a mix of oncocytic and clear cells could additionally be seen, as clearing outcomes from degeneration of the oncocytic cells. Lymphovascular invasion is famous with tumor cells inside a vascular area, related to squamous metaplasia. The gland is agency, with white streaks and a gritty minimize consistency, and an ill-defined border, if a dominant mass is noted. Total thyroidectomy, lymph node dissection, and radioablative remedy will yield a superb long-term prognosis despite the "biologically" aggressive clinical presentation. Lung metastases occur in as a lot as 25% of patients, necessitating shut and careful patient follow-up. When this cell type is the dominant finding in the neoplasm (range from 30% to 70%, but larger than 30% of the tumor space yields the most consistent correlation with outcome), the sufferers tend to be older (> 60 years), with an increased proportion of males, and the tumor tends to be massive (> 5 cm), exhibiting extrathyroidal extension. There is an increased incidence of lymph node metastasis and hematogenous spread to bone and lung, with a bent for local recurrence and invasion into adjoining constructions. Surgery and adjuvant remedy are essential, with a worse prognosis than classic papillary carcinoma. Tumors are usually massive (> 5 cm) and encapsulated, however have intra- and extrathyroidal spread. There is distinguished nuclear stratification of elongated nuclei with coarse and heavy chromatin deposition, distinctly completely different from classic papillary carcinoma. If the patient is older with a big tumor that has extrathyroidal extension, extra aggressive surgery and radioablative remedy could also be needed. The prognosis is worse than for classic papillary carcinoma, although it might be extra a characteristic of infiltration than cytologic variant. Some examples of columnar variant histologically overlap with the more indolent cribriform-morular variant (discussed below). In these very unusual and weird histologic variants, performing selected immunohistochemistry research (such as -catenin in circumstances with squamous metaplasia) may be of worth. There are often whorls or morules composed of spindle cells with out keratinization, exhibiting an optically clear nucleus. Prominent subnuclear vacuoles are seen in cells arranged in a cribriform structure. These constructions are lined by follicular cells that have a hobnail appearance, with apically positioned nuclei showing prominent nucleoli.
Cheap amlodipine 5 mg with amexBenefits must outweigh risks if ifosfamide is used in sufferers with pre-existing renal impairment or lowered nephron reserve prehypertension que es amlodipine 10 mg cheap. Glomerular and tubular disorders of renal operate are widespread and may become obvious during remedy or months and years after stopping treatment blood pressure chart paediatrics discount 10 mg amlodipine with mastercard. Risk of hemorrhagic cystitis is dose-dependent and will increase with the administration of single high doses in comparability with arteria bologna buy amlodipine 5 mg without prescription fractionated administration blood pressure gauge 10 mg amlodipine generic fast delivery. Past or concomitant radiation of the bladder or busulfan therapy may increase threat. Risk is dose dependent and is increased with prior or concomitant treatment with other cardiotoxic brokers or radiation of the cardiac region and, possibly, renal impairment. Blurred imaginative and prescient, coma, confusion, extrapyramidal signs, hallucinations, psychotic behavior, seizures, somnolence, and urinary incontinence have been reported. Neurotoxicity might seem inside a quantity of hours to a quantity of days after the first administration and often resolves inside forty eight to seventy two hours of discontinuing ifosfamide, though signs might persist. Fanconi syndrome, renal rickets, and growth retardation have been reported in pediatric patients. Prepubescent females might turn into sterile or are in danger for developing premature menopause. Prepubescent males may not develop secondary sexual traits normally and may have oligospermia or azoospermia. Post-Marketing: Anaphylaxis; angioedema; benign and malignant neoplasms; hematotoxicity. Imiglucerase: Adults and pediatric sufferers over 2 years of age: Individualized to every affected person based mostly on the severity of illness and patient response. Velaglucerase alfa: Adult and pediatric sufferers four years of age and older na�ve to enzyme alternative therapy: 60 units/kg each other week. Patients presently being treated with a steady dose of imiglucerase could also be switched to velaglucerase alfa at that same dose 2 weeks after the final imiglucerase dose. Imiglucerase: To make the most of every bottle totally and cut back waste, a single dose may be elevated or decreased barely so lengthy as the whole monthly dose remains unaltered. Weight in kg three dose/kg desired 4 (200 or 400 units/vial) 5 # of vials required A 60-kg man requiring 60 units/kg would require three,600 items. Number of vials required would be 18 vials at 200 units/vial or 9 vials at 400 units/vial. Imiglucerase: Adjust variety of vials up or down inside month-to-month dose requirement to absolutely make the most of every vial. Let stand for a number of minutes to enable product to dissolve and bubbles to dissipate. Return of unsuitable vials (reconstituted, before reconstitution, or expired) may be licensed; contact manufacturer. Should be promptly diluted after reconstitution but has been shown to be Copyright � 2021 by Elsevier Inc. Velaglucerase alfa: Refrigerate at 2� to 8� C (36� to 46� F) in carton before use. Immediate use is preferred, but reconstituted and absolutely diluted solutions are secure for up to 24 hours if refrigerated and protected from gentle. Velaglucerase alfa is a hydrolytic lysosomal glucocerebroside-specific enzyme and is produced by gene activation technology in a human fibroblast cell line. Gaucher illness is characterized by a functional deficiency in beta-glucocerebrosidase enzymatic activity and the resultant accumulation of lipid glucocerebroside in tissue macrophages (Gaucher cells). These cells are found within the liver, spleen, bone marrow, and infrequently within the lung, kidney, and intestine. These agents act like glucocerebrosidase, catalyzing the hydrolysis of glucocerebroside to glucose and ceramide. Increase in appetite and vitality degree and improvement in hemoglobin are sometimes the first observable effects and may happen in 2 to 4 months. Replenishment of bone marrow and bettering mineralization of bone may take several years. Velaglucerase alfa: Long-term enzyme substitute therapy for pediatric and grownup sufferers with Type 1 Gaucher illness. Most sufferers who develop antibodies to imiglucerase achieve this inside 12 months of treatment. Patients with antibodies to imiglucerase are at elevated threat for growing hypersensiCopyright � 2021 by Elsevier Inc. Evaluate sufferers with respiratory signs within the absence of fever for the presence of pulmonary hypertension. Velaglucerase alfa: Hypersensitivity reactions, together with anaphylaxis, have occurred. Patients who develop hypersensitivity reactions to velaglucerase may be premedicated (see Usual Dose and/or Antidote). Frequency determined by patient response; extra frequent when figuring out response to initial dose and when dose is being adjusted. Blood tests shall be carried out more incessantly because anemia is the primary symptom to improve. Maternal/Child: Both preparations: Safety for use throughout breast-feeding not established. Not identified if Imiglucerase: Use in pregnancy provided that potential profit justifies the risk. Velaglucerase alfa: Differences in responses and side effects between elderly and youthful patients not identified; see Dose Adjustments. In addition, belly discomfort; backache; burning, discomfort, and pruritus at injection website; chills; diarrhea; dizziness; fatigue; fever; hypotension (mild); nausea; peripheral edema (transient); swelling or sterile abscess at venipuncture site; tachycardia; and vomiting had been reported. Other reported side effects embrace bone ache, flushing, hypertension, hypotension, rash, tachycardia, urticaria, and vomiting. Based on the severity of the reaction, temporarily interrupt or discontinue infusion for scientific proof of hypersensitivity response. Patients have successfully continued therapy after mild hypersensitivity or infusion reactions with pretreatment with antipyretics, antihistamines. The dosage suggestions within the following chart symbolize the amount of imipenem to be administered. Cystic fibrosis and regular renal function: Higher doses as a lot as 100 mg/kg/day have been used. Shake properly and switch the ensuing suspension to 100 mL of the identical infusion answer. Rinse vial with a further 10 mL of infusion resolution to guarantee full transfer of vial contents to the infusion answer. Neonatal dilution: Use preservative-free options for reconstitution of neonatal doses. An in-house research documented compatibility of the ultimate diluted resolution with a 0. Diluted solutions are secure at room temperature for 4 hours after preparation or 24 hours if refrigerated. Imipenem is a carbapenem antibiotic; cilastatin inhibits the kidney enzyme answerable for the metabolism of imipenem. Has a high diploma of stability in the presence of beta-lactamases produced by gram-negative and gram-positive bacteria. Unlabeled makes use of: Treatment of cystic fibrosis exacerbations, febrile neutropenia, and melioidosis (a uncommon an infection in humans and animals). More likely in sufferers with a historical past of sensitivity to a number of allergens; acquire a careful historical past. Consider in sufferers who present with diarrhea throughout or after therapy with imipenem-cilastatin. Carbapenems may reduce serum valproic acid concentrations to subtherapeutic ranges, resulting in lack of seizure control. Increasing the dose of valproic acid is most likely not adequate to overcome this interaction. Concomitant use of imipenem and valproic acid/ divalproex sodium is generally not beneficial.
Stemless Carlina Root (Carlina). Amlodipine. - How does Carlina work?
- Dosing considerations for Carlina.
- Are there safety concerns?
- What is Carlina?
- Gallbladder disease; poor digestion; spasms of the esophagus, stomach, and intestines; skin problems; wounds; cancer of the tongue; herpes; toothache; causing sweating; and use as a diuretic, tonic, or gargle.
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96142
Buy cheap amlodipine 5 mg lineAn infiltrative development pattern is defined by bone and gentle tissue invasion (assessed by imaging or histology) and is recognized in many circumstances heart attack normal blood pressure amlodipine 5 mg effective. Nearly all tumors are World Health Organization grade I blood pressure medication given during pregnancy amlodipine 2.5 mg buy generic on-line, with the meningothelial (syncytial) and psammomatous variants arterial hypertension treatment discount 5 mg amlodipine with visa, respectively blood pressure 9040 amlodipine 2.5 mg amex, the most regularly occurring. A middle ear adenoma has a more organoid growth with neuroendocrine nuclear options and powerful keratin and neuroendocrine immunoreactivity. Paraganglioma shows a zellballen (nested) architecture with basophilic cells and a distinctive immunoprofile: chromogranin-positive paraganglia cells and S100 protein�positive supporting sustentacular cells. A meningocele, or protrusion of the meninges via a bony defect, can happen in the center ear and temporal bone, but these are histologically cystic lesions with a connection to the central nervous system. In spite of further surgical procedure, sometimes sufferers will die with disease (although "from" disease is tough to determine). In the case of skull base involvement, surgical approaches are complicated and challenging (transpetrosal, subtemporal, transtentorial). Adjuvant radiation therapy is utilized in poor surgical candidates or in cases of incomplete surgical resection. Patients present with unilateral illness and associated tinnitus, fullness or strain, otitis media, and conductive hearing loss, especially if the ossicular chain is involved. In early levels, otoscopy shows an intact tympanic membrane with a darkish brownish-red mass behind it. The tumor may later expand to and contain the ossicular chain, thus causing conductive listening to loss, and may even penetrate the tympanic membrane. Because they tend to encase the ossicular chain, the tumor is often peeled away from the bone upon resection. Therefore, surgical specimens are highly fragmented and encompass whitish-yellow to grey, soft to rubbery tissue. The nuclei are most likely to be round to oval, eccentrically placed ("plasmacytoid"), with minimal pleomorphism and "salt and pepper" chromatin distribution. An "infiltrative" sample is characterized by small irregular teams and strands of cells in a moderately desmoplastic stroma. The cells tend to be smaller than those inside the different patterns and have a higher nuclear to cytoplasmic ratio. Additional options could embody a concurrent cholesteatoma and/or cholesterol granuloma. However, the anatomic site of origin makes this a singular tumor, distinctly separable from the opposite lesions by histology and immunohistochemistry. Because glandular (mucosal) metaplasia of the middle ear epithelium is common in persistent irritation, such as otitis media, adenoma would appear to be the benign neoplastic counterpart of this reactive process. A Grimelius stain could reveal granular cytoplasmic positivity on the base of the cells (periphery of the glands), corresponding to the placement of the neurosecretory granules by electron microscopy. Recurrence (persistence) is likely to develop in 15% of sufferers, particularly when the ossicular chain is involved but not eliminated. Facial nerve paralysis or paresthesia is usually mass-related compression quite than invasion, whereas parotid gland involvement normally represents direct extension somewhat than metastatic disease. Although controversial, there appears to be an especially low threat of metastatic disease. There is a large age range at presentation, although most sufferers are between 30 and 40 years. The most common signs include ipsilateral listening to loss (sensorineural > conductive, although could be mixed), tinnitus, facial nerve palsy, and vestibular dysfunction (vertigo, ataxia) resembling M�ni�re illness. Tumor expansion into neighboring structures (especially middle and posterior cranial fossae and cerebellopontine angle) may also be seen. These cells comprise uniformly spherical to oval nuclei with coarse nuclear chromatin deposition and eosinophilic, granular cytoplasm with indistinct cell membranes. Granulation tissue, hemosiderin, persistent inflammation, and ldl cholesterol clefts could also be related. The prognosis depends on the extent of the disease, with death often reported because of destruction of important structures, as a outcome of the indolent however progressive course. Metastatic carcinomas (lung, kidney, colon, prostate) may be distinguished with the assistance of immunohistochemistry. How to address small- and medium-sized acoustic neuromas with listening to: a systematic review and choice analysis. Less than 1% cerebrospinal fluid leakage in 1,803 translabyrinthine vestibular schwannoma surgical procedure circumstances. Management of vestibular schwannomas in young patients-comparison of scientific options and consequence with grownup patients. Management of one thousand vestibular schwannomas (acoustic neuromas): surgical administration and outcomes with an emphasis on issues and the means to avoid them. Surgical administration of jugular foramen schwannomas with hearing and facial nerve operate preservation: a collection of 23 cases and evaluation of the literature. Middle ear adenomas stain for two cell populations and lack myoepithelial cell differentiation. Pleomorphic adenoma presenting with conductive listening to loss within the ear canal: a case report and review of the literature. Polygonal cells with ceroid granules and myoepithelial cells in fantastic needle aspiration cytology of ceruminous adenoma. Middle-ear ceruminous adenoma as a uncommon explanation for listening to loss and vertigo: case reviews. Ceruminous adenomas: a clinicopathologic research of forty one circumstances with a evaluation of the literature. Detection of cloncla lymphoid receptor gene rearrangements in Langerhans cell histiocytosis. Differentiating pediatric rhabdomyosarcoma and Langerhans cell histiocytosis of the temporal bone by imaging appearance. Langerhans cell histiocytosis within the paediatric inhabitants: presentation and remedy of head and neck manifestations. Immunohistochemcial expression of langerin in Langerhans cell histiocytosis and non-Langerhans cell histiocytic disorders. Langerhans cell histiocytosis of the temporal bone: A review of 29 circumstances at a single heart. Surgical administration of glomus jugulare tumors: a proposal for method choice based on tumor relationships with the facial nerve. Natural historical past of glomus jugulare: a review of 16 tumors managed with primary statement. Inherited mutations in pheochromocytoma and paraganglioma: why all patients must be supplied genetic testing. Clinical views regarding sufferers with internal auditory canal or cerebellopontine angle lesions: surgical and radiation oncology perspectives. Surgical management of extensive jugular paragangliomas: 10-year-experience with a large cohort of sufferers in China. Carcinoid tumor of the center ear: clinical options, recurrences, and metastases. Intracanalicular meningioma: scientific features, radiologic findings, and surgical management. Meningiomas presenting in the temporal bone: the pathways of unfold from an intracranial web site of origin. Transpetrosal approaches for meningiomas of the posterior facet of the petrous bone Results in 43 consecutive sufferers. A clinicopathological examine of 15 sufferers with neuroglial heterotopias and encephaloceles of the middle ear and mastoid area. Middle ear meningiomas: a case sequence reviewing the scientific presentation, radiologic features, and up to date administration of a rare temporal bone pathology. Primary ear and temporal bone meningiomas: a clinicopathologic examine of 36 cases with a evaluation of the literature. Endolymphatic sac tumor (low-grade papillary adenocarcinoma) of the temporal bone. Low-grade adenocarcinoma of possible endolymphatic sac origin: a clinicopathologic research of 20 circumstances. Endolymphatic sac tumor related to a von Hippel-Lindau disease affected person: an immunohistochemical research.
2.5 mg amlodipine free shippingDeferoxamine is an iron chelating agent and may be useful in iron toxicity or overdose blood pressure chart heart rate 10 mg amlodipine cheap free shipping. Administer on 5 totally different days over a 14-day interval to a total cumulative dose of 1 blood pressure 9870 amlodipine 10 mg order free shipping,000 mg hypertension zinc amlodipine 5 mg order without a prescription. In dialysis sufferers hypertension 180120 amlodipine 5 mg buy fast delivery, administer into the dialysis line during the dialysis session. Infusion in adults: this methodology of administration might scale back the danger of hypotensive episodes. Alternately could also be diluted and given as an infusion equally distributed over a minimum of 15 minutes. Has also been administered as an infusion in a 500-mg dose equally distributed over three. Iron is critical for normal hemoglobin synthesis to keep oxygen transport and is important for various different processes. Following intravenous administration, iron sucrose is dissociated by the reticuloendothelial system into iron and sucrose. Significant will increase in serum iron and ferritin and important decreases in total iron-binding capacity happen inside four weeks of starting iron sucrose treatment. Recumbent position during and after administration might assist to stop postural hypotension. Hypotensive results may be additive to transient hypotension during dialysis and/or from too-rapid fee of administration. No causal relationship to medicine might be established; it might be a complication of prematurity in very-low-birthweight infants. May reduce the absorption of concomitantly administered oral iron preparations; concurrent use not recommended. Other unwanted side effects various in accordance with the sort of chronic kidney disease patient who was receiving iron sucrose. Pediatric sufferers: Arteriovenous fistula thrombosis, cough, dizziness, fever, headache, hypertension, hypotension, nausea, peritonitis, respiratory tract viral an infection, and vomiting occurred. If acute toxicity is seen, it could current as abdominal and muscle pain, cardiovascular collapse, dizziness, dyspnea, edema, headache, hemosiderosis, hypotension, joint aches, nausea, pale eyes, paresthesia, sedation, vomiting. Institute antifungal remedy and modify primarily based on outcomes of culture and lab studies. Available as a lyophilized powder containing 372 mg isavuconazonium sulfate (equivalent to 200 mg isavuconazole). Diluted answer could have visible translucent to white particulates, which shall be eliminated by in-line filtration. Reconstituted solution ought to be additional diluted and used immediately but could also be saved under 25� C for a maximum of 1 hour earlier than additional dilution. Administer a single dose as an infusion equally distributed over a minimum of 60 minutes. Administer via an infusion set that contains a sterile, nonpyrogenic, in-line filter (pore dimension of 0. Acts by inhibiting the synthesis of ergosterol, a key part of fungal cell membranes. Rapidly hydrolyzed in blood to isavuconazole by esterases, predominantly by butylcholinesterase. Treatment of invasive aspergillosis and invasive mucormycosis in patients 18 years of age and older. Relevance of cross-resistance to clinical outcome has not been totally characterized. Monitor: Obtain specimens for fungal culture and different relevant lab research (including histopathology) to isolate and establish causative organism(s) before initiating therapy. Monitor more incessantly in sufferers who develop irregular liver function checks and when treating sufferers with extreme hepatic impairment. Use throughout being pregnant provided that the potential benefit to the affected person outweighs the risk to the fetus. Monitor drug concentrations of these drugs and/or drug-related toxicities and modify doses as needed. Hepatic antagonistic drug reactions, infusion-related or hypersensitivity reactions, and embryo-fetal toxicity are thought of essentially the most serious. Abdominal pain, acute respiratory failure, anxiety, chest pain, decreased urge for food, delirium, dyspepsia, fatigue, hypomagnesemia, hypotension, injection website reaction, insomnia, pruritus, rash, and renal failure have also been reported. If a hypersensitivity reaction, infusion response, or severe cutaneous reaction happens, discontinue the infusion and treat as indicated. Discontinue isavuconazonium if scientific S/S in preserving with liver disease develop that may be attributable to isavuconazonium. Recommended Isoproterenol Dose for Adults With Atropine-Resistant Hemodynamically Significant Bradycardia, Heart Block, Adams-Stokes Attacks, and Cardiac Arrest Route of Administration Bolus intravenous injection Intravenous infusion Preparation of Dilution Dilute 1 mL (0. Recommended Isoproterenol Dose for Adults With Bronchospasm Occurring During Anesthesia Route of Administration Bolus intravenous injection Preparation of Dilution Dilute 1 mL (0. Diagnosis of mitral regurgitation (unlabeled): four mcg/min as an infusion (1 mL/min of a 4 mcg/mL dilution). Diagnosis of coronary artery disease or lesions (unlabeled): 1 to 3 mcg/min as an infusion (0. Lower-end initial doses could also be applicable in the elderly; contemplate the potential for decreased organ operate and concomitant illness or drug remedy. Another supply cites no vital loss in drug potency in several studies using various types and sizes of filters from 0. Storage: Store between 8� and 15� C (46� to 59� F) unless otherwise specified by producer. Isoproterenol (Isuprel) Infusion Rates 1 mg in 500 mL D5W (2 mcg/mL) mcg/hr a hundred and twenty 300 600 900 1,200 1,500 1,800 mL/min 1 2. Has optimistic inotropic and chronotropic actions stronger than those of epinephrine. Stimulates only the upper ventricular foci, permitting a extra normal cardiac pacemaker to take over, thus suppressing ectopic pacemaker activity. Decreases peripheral vascular resistance by stress-free arterial easy muscle and is a handiest bronchial clean muscle relaxant. Tachyarrhythmias, patients with tachycardia or coronary heart block attributable to digoxin intoxication, angina pectoris, ventricular arrhythmias that require inotropic therapy. Risks of cardiac toxicity could additionally be elevated by different factors similar to acidosis, hypoxemia, coadministration of corticosteroids or methylxanthines. May be used to treat tachycardia caused by isoproterenol, however tachycardia and hypotension secondary to peripheral vasodilation could happen. Anginal ache, cardiac arrhythmias, flushing, headache, hyperglycemia, hypokalemia, nausea, nervousness, palpitations, sweating, tachycardia, vomiting. Cardiac dilation, marked hypotension, pulmonary edema, and death may happen with prolonged use or overdose. For unintentional overdose, discontinue drug immediately, resuscitate and maintain affected person, and notify physician. Patients who experience a hypersensitivity reaction require premedication with a corticosteroid. Administered alone or in combination with capecitabine (Xeloda) 1,000 mg/M2 twice daily for 2 weeks adopted by 1 week of rest. Dosage recommendations are for the first course of remedy; additional decreases in subsequent programs ought to be based mostly on particular person tolerance. If the sturdy inhibitor is discontinued, await a minimal of 1 week earlier than adjusting the ixabepilone dose upward to the indicated dose. Increase infusion duration of 60 mg/M2 dose to four hours and monitor patient carefully for toxicity. Available as a 15-mg or 45-mg Ixempra Kit that contains two vials; one vial contains the indicated amount of ixabepilone, and the other incorporates a manufacturer-supplied diluent. Filter: Must be administered via an in-line filter with a microporous membrane of zero.
Buy 2.5 mg amlodipine otcSafety of administering stay or live-attenuated vaccines in exposed infants is unknown prehypertension meaning in urdu generic 2.5 mg amlodipine overnight delivery. Arthralgia arteria alveolaris superior posterior order amlodipine 5 mg with mastercard, again pain blood pressure medication sore joints amlodipine 5 mg order overnight delivery, bronchitis blood pressure up and down all day amlodipine 10 mg cheap on line, cough, fatigue, fever, headache, influenza, nasopharyngitis, nausea, oropharyngeal ache, pain in extremities, pruritus, rash, sinusitis, and higher respiratory tract infection are most common. Infusion-related reactions and hypersensitivity reactions, including anaphylaxis, have occurred. Discontinue infusion if any S/S of a severe hypersensitivity or infusion response happen. Treat with epinephrine, corticosteroids, diphenhydramine, bronchodilators, and oxygen as indicated. In medical trials, sufferers with mild to moderate infusion-related reactions or hypersensitivity reactions were pretreated with normal medical remedy. It inhibits calcium (and presumably sodium) ion inflow via slow channels into conductile and contractile myocardial cells and vascular smooth muscle cells. Reduces myocardial contractility, afterload, arterial strain, systemic vascular resistance, and oxygen demand. Hemodynamic results last about 20 minutes, but antiarrhythmic effects may last as long as 6 hours. A small fraction (less than 1%) of patients could respond with life-threatening adverse responses, together with speedy ventricular rate in atrial flutter/fibrillation with an adjunct bypass tract, marked hypotension, or extreme bradycardia/asystole. Maternal/Child: Category C: safety to be used in pregnancy not but established; use solely when clearly indicated. Concurrent use will increase serum concentrations of ivabradine, which may exacerbate bradycardia and conduction disturbances. In sufferers receiving verapamil, limit dose of simvastatin to 10 mg every day and restrict lovastatin dose to forty mg daily. Discontinue verapamil and notify physician promptly if hypotension, bradycardia, or second- or third-degree heart block occurs. Norepinephrine (Levarterenol), calcium chloride, or dopamine will reverse hypotension. The greatest linear dimension of the lesion is estimated by fluorescein angiography and colour fundus photography. The therapy spot measurement should be 1,000 microns larger than the greatest linear dimension of the lesion on the retina to allow a 500-micron border. The nasal fringe of the treatment spot must be positioned at least 200 microns from the temporal edge of the optic disc. Second stage: Activation of verteporfin utilizing a really helpful mild dose of fifty J/cm2 of neovascular lesion administered at an intensity of 600 mW/cm2 over 83 seconds. Initiate 689 6 3 nm wavelength laser gentle delivery quarter-hour after the start of the verteporfin infusion. Light is delivered to the retina as a single round spot by way of a fiber optic and a slit lamp, utilizing an acceptable ophthalmic magnification lens. Light dose, mild intensity, ophthalmic lens magnification issue, and zoom lens setting are important parameters for the suitable supply of sunshine to the predetermined remedy spot. Concurrent bilateral remedy: In sufferers who current with eligible lesions in each eyes with out prior verteporfin therapy, treat only one eye (the most aggressive lesion) during the first course. One week after the first course, if no important issues of safety are recognized, the second eye can be treated, using the identical therapy regimen together with a verteporfin infusion and light-weight activation. Approximately 3 months later, both eyes could be evaluated, and concurrent therapy following a brand new verteporfin infusion may be started if each lesions still show proof of leakage. When treating each eyes concurrently, the extra aggressive lesion must be handled first, at quarter-hour after the beginning of infusion. Immediately at the end of sunshine utility to the first eye, the laser settings should be adjusted to introduce the therapy parameters for the second eye, with the same light dose and depth as for the primary eye, starting no later than 20 minutes from the beginning of the infusion. Withdraw the specified dose from the vial and additional dilute with D5W to a total infusion quantity of 30 mL. Reconstituted and diluted answer have to be protected against gentle and used inside 4 hours. A 30-mL infusion equally distributed over 10 minutes (3 mL/min) utilizing an acceptable syringe pump and a 1. Endothelial cells of the irregular choroidal blood vessels, which have high concentrations of lipoprotein receptors, take up the lipoprotein-verteporfin complicated. Light activation in the presence of O2 induces a photochemical reaction, generating extremely reactive singlet oxygen and reactive oxygen radicals that cause native injury to the neovascular endothelium. The broken endothelium releases procoagulant and vasoactive elements via the lipo-oxygenase (leukotriene) and cyclo-oxygenase (eicosanoids corresponding to thromboxane) pathways, resulting in platelet aggregation, fibrin clot formation, vasoconstriction, and in the end, vessel occlusion. Verteporfin appears to preferentially accumulate in neovasculature, together with choroidal neovasculature. Therefore, there may be collateral injury to retinal buildings following photoactivation. It is metabolized to a small extent by liver and plasma esterases and is eradicated primarily by the fecal route as unchanged drug. Patients with porphyria or a known hypersensitivity to any element of this preparation. Protection from gentle shall be needed if accidental publicity or overexposure happens. Facilities for monitoring the patient and responding to any medical emergency should be obtainable. If emergency surgical procedure is important inside 48 hours after therapy, as a lot of the internal tissue as possible must be protected against intense mild. If extravasation occurs, the infusion should be stopped immediately and chilly compresses applied. The extravasation space must be thoroughly protected against direct mild until the swelling and discoloration have faded to be able to forestall the incidence of a neighborhood burn, which might be extreme. Verteporfin has caused a concentration-dependent increase in complement activation in human blood in vitro. S/S in keeping with complement activation (chest pain, dyspnea, flushing, syncope) have been reported. Patient Education: n Must observe precautions to avoid exposure of pores and skin and eyes to direct sunlight or bright indoor light for 5 days. Photosensitivity is as a outcome of of residual drug, which is present in all components of the pores and skin. Avoid brilliant indoor gentle from examination lamps, dental lamps, working room lamps, bright halogen lighting, and unshaded gentle bulbs. Limit time outside to needed excursions and utterly cowl body with clothing and shade face before going out. Maternal/Child: Category C: use throughout being pregnant provided that advantages justify potential danger to fetus. Elderly: Reduced treatment effect was seen with rising age (75 years of age or older). Based on the mechanism of motion of verteporfin, many medication used concomitantly could affect the effect of verteporfin therapy. The most regularly reported unwanted effects are headache, injection site reactions. Less incessantly reported side effects embody abnormal white blood cell depend (decreased or increased), albuminuria, anemia, arthralgia, arthrosis, asthenia, atrial fibrillation, again pain (primarily during infusion), blepharitis, cataracts, chest ache, conjunctivitis, constipation, decreased listening to, diplopia, dizziness, dry eyes, dyspnea, eczema, elevated liver function exams, eye hemorrhage (subconjunctival, subretinal, or vitreous), fever, flu-like syndrome, flushing, hyperesthesia, hypersensitivity reactions, hypertension, increased creatinine, lacrimation disorder, malaise, myasthenia, Copyright � 2021 by Elsevier Inc. Overdose: Overdose of drug and/or gentle may lead to nonperfusion of normal retinal vessels with the potential of severe lower in vision that could be permanent. May also result in prolongation of the time during which the patient will be photosensitive. In the occasion of an overdose of drug and/or gentle, prolong the photosensitivity precautions for a time proportional to the overdose. After the first hour, increase the infusion fee as tolerated in order to complete the infusion over the next 3 hours; see Rate of Administration. Available as a colorless to slightly yellow liquid in a single-dose vial containing 10 mg/5 mL (2 mg/mL). Volume (mL) of calculated dose 5 Total dose (mg) � 2 mg/mL concentration answer. Select an empty infusion bag based mostly on the total quantity of the final resolution as a 1:1 dilution.
Buy 2.5 mg amlodipine with visaThe incidence of thyroid disorders locally: a twenty-year follow-up of the Whickham survey zantac blood pressure medication generic amlodipine 2.5 mg otc. A perspective on human autoimmune thyroid disease: is there an abnormality of the target cell which predisposes to the dysfunction Nodular goiter and goiter nodules: where iodine deficiency falls wanting explaining the details blood pressure medication how long to take effect amlodipine 2.5 mg low cost. Natural heterogeneity of thyroid cells: the idea for understanding thyroid perform and nodular goiter development heart attack 50 damage generic amlodipine 10 mg with visa. The use of fine-needle aspiration under ultrasound steerage to assess the danger of malignancy in sufferers with a multinodular goiter blood pressure j curve 10 mg amlodipine discount overnight delivery. Genotype-phenotype correlations of dyshormonogenetic goiter in youngsters and adolescents from South India. Minimally invasive follicular thyroid carcinoma developed in dyshormonogenetic multinodular goiter due to thyroid peroxidase gene mutation. Amyloid goiter: cytomorphological features and differential diagnosis on nice needle aspiration cytology: a case report. Minocycline and the thyroid: antithyroid results of the drug, and the role of thyroid peroxidase in minocycline-induced black pigmentation of the gland. Interrelationships between age, thyroid volume, thyroid nodularity, and thyroid function in patients with sporadic non-toxic goiter. Patients are usually euthyroid and solely not often develop hyperfunction ("poisonous adenoma") or hypofunction. Neck ache or pressure may be reported if bleeding into the tumor has occurred or due to compressive symptoms in large tumors. Color Doppler gives a "spoke and wheel" look of peripheral blood vessels extending toward the middle of the lesion. Cystic change, degeneration, calcification, and infarction are frequent and should alter the physical look. If the tumor appears macroscopically homogeneous after being bivalved, then the center of the tumor is of much less curiosity and must be sampled only representatively. The tumor is serially sectioned perpendicular to the capsule, making 2- to 3-mm thick sections. Then the very periphery of the tumor to capsule to parenchymal interface is embedded. Adenomas are often spherical to spherical, measuring about 1 to 3 cm on common, although this can be quite variable relying on scientific presentation (palpable versus incidental radiographic feature). If the capsule could be very thick, additional sections ought to be evaluated to exclude a carcinoma. The web site of puncture often has a "sharp edge" of transgression, suggesting a mechanical device rather than biologic aggression. The cells are arranged in quite lots of patterns with a variable quantity of colloid, often distinctive from the encircling parenchyma. The follicles are usually uniform with a single architectural pattern predominating. Delicate capillaries are simply identified, however intratumoral fibrosis is uncommon. There is a low nuclear:cytoplasmic ratio with well-defined cell borders within the cuboidal to columnar cells. The nuclei are often aligned in an orderly arrangement alongside the basal facet of the cell. There is ample eosinophilic, granular cytoplasm surrounding nuclei that are generally round and common, sometimes with outstanding nucleoli. Oncocytic tumors should be interpreted with caution owing to excessive background and nonspecific staining. After adequacy is assessed (five or six follicular epithelial groups of at least 10 epithelial cells per group), a follicular neoplasm may be favored over an adenomatoid nodule (colloid goiter). The epithelial groups are arranged as small spherical aggregates surrounding a colloid droplet. Adenomatoid nodules are most likely to have cellular variability and infrequently show in depth degenerative modifications. Scant colloid is present (A and C, air-dried, Diff-Quik stain; B and D, alcohol-fixed, Papanicolaou stain). With that stated, adenomatoid nodules are often a quantity of, lack a capsule with smooth muscle� walled vessels, and often have far more abundant colloid and degenerative modifications than an adenoma. However, features that increase the suspicion of carcinoma embody a remarkably thickened fibrous capsule, increased cellularity (especially at the periphery of the tumor), elevated mitotic exercise, atypical mitotic figures, and tumor necrosis. However, additional architectural and cytomorphologic features of papillary carcinoma must be current before making the analysis: invasive development, intratumoral fibrosis, thick eosinophilic colloid, and the characteristic nuclear options of enlargement, crowding, irregular placement around the follicle, grooves, folds, and contour irregularities, with chromatin clearing and margination. Nuclear options of papillary carcinoma alone in a follicular neoplasm are not adequate to render a analysis of papillary carcinoma; structure, sample of growth, cytoplasmic qualities, and invasion must be taken into consideration. The nodule may be palpable or incidentally found on imaging carried out for one more indication. Thus, the incidence in the basic population is estimated to be roughly 1 in one hundred,000. Tumors are circumscribed or grossly encapsulated and often 2 to 4 cm in diameter, however they may be a lot larger. Use of a 3-point scoring system to consider the nuclei could also be helpful: 1 point is given for nuclear enlargement, crowding, and overlap; 1 level for nuclear contour irregularity including grooves, folds, and pseudoinclusions; and 1 point for nuclear clearing, margination, or glassy nuclei. Use of the previously described 3-point system for scoring nuclear features (with a rating of 2 or 3 considered positive) may be helpful. The remaining cases are often categorised as suspicious for malignancy (Bethesda category V). The molecular alterations overlap with different benign and malignant thyroid neoplasms. Extremely rare examples with invasive progress and metastasis have been described (hyalinizing trabecular carcinoma). Ultrasonography shows a strong nodule with hypoechoic or heterogeneous echogenicity. Vascular and/ or capsular invasion is nearly all the time absent; when current, it indicates a hyalinizing trabecular carcinoma. The nests are fashioned by a dense, heavily hyalinized eosinophilic fibrovascular stroma. The cells are medium to giant, polygonal to fusiform, with variable cytoplasm surrounding the oval to elongated nuclei. Multiple intranuclear cytoplasmic inclusions (arrows) and perinucleolar halos are present. Strong membranous Ki-67 (with the Aspirates are mobile, with cohesive clusters of cells and ample cytoplasm. Nuclei are elongated with evenly dispersed chromatin, intranuclear cytoplasmic inclusions, and nuclear grooves. When current, this materials is usually radially oriented around cells, accounting for the hyalinized nature of this tumor. The dense, basement membrane materials could be seen in both photographs, though highlighted in magenta-purple with the Diff-Quik preparation (B). Paraganglioma, rare in the thyroid, could be readily ruled out by its attribute immunophenotype (neuroendocrine markers positive, with S100 protein staining the sustentacular cells; cytokeratin negative). A trabecular sample of development could be seen in papillary, medullary, and follicular neoplasms. Follicular carcinoma with trabecular structure, by definition, could have invasion. Patients vary from newborn to eighty five years of age at initial presentation, although the height and median fall inside the new child period. The average age, however, is skewed by older patients who normally have malignant teratomas. In fact, more than 90% of the tumors within the neonatal group will be benign teratomas, whereas 50% or more of the child/ grownup group will have malignant teratomas. All patients present with an anterior neck mass, typically reaching a significant size. Although data are restricted, in the few welldocumented instances, metastases happen in tumors that show invasive growth (capsular and lymphovascular invasion).
Amlodipine 5 mg without a prescriptionFor the most half pulse pressure different in each arm safe 10 mg amlodipine, monographs which are supposedly up to date to the newer specs present little steering prehypertension 139 amlodipine 5 mg buy generic on-line. No drug must be used during pregnancy except clearly wanted and the risks to the fetus are outweighed by the advantages to the mom hypertension questions and answers 10 mg amlodipine cheap otc. Consider all men and women able to conception when any drug in Category D or Category X is to be administered arteria rectalis media 10 mg amlodipine purchase fast delivery. Discuss birth control choices to avoid pregnancy if a selected drug in these categories must be administered. This itemizing has been expanded and updated by these organizations and is too expansive to be included in an appendix. Department of Health and Human Services, the National Institutes of Health, and the National Cancer Institute. Nonhormonal contraception reduces the potential for drug interactions, but compliance is crucial. Alternate methods of dental hygiene may be needed should your gums turn out to be tender, infected, or bleed. Confirm those that might be a special downside for you and talk about solutions and expectations. Report signs similar to chills, fever, cough, hoarseness, lower again or aspect pain, painful or tough urination. Available as a clear, colorless solution in a single-dose vial containing 5 mg/2 mL (2. Amisulpride is a selective dopamine-2 (D2) and dopamine-3 (D3) receptor antagonist. Studies in a quantity of species indicate that D3 receptors in the area postrema also play a task in emesis. Amisulpride is considerably excreted by the kidneys, and sufferers with severe renal impairment may have increased systemic publicity and an elevated risk of adverse reactions. Contact supplier instantly for light-headedness, a syncopal episode, or a perceived change in coronary heart price. Review all prescription and nonprescription medications with a health care skilled. Consider pumping and discarding milk for 48 hours after amisulpride administration to cut back toddler exposure. Amisulpride is substantially excreted by the kidneys, and the danger of antagonistic reactions may be higher in patients with impaired renal operate. Post-Marketing: the following antagonistic reactions have been reported throughout postapproval persistent oral use of amisulpride exterior of the United States. Management includes cardiac monitoring and treatment of severe extrapyramidal symptoms. Dosage adjustment in sufferers with any degree of hepatic impairment is unnecessary. No dosage adjustment is beneficial in patients with mild, reasonable, or extreme renal impairment. The 60-hour infusion will generally require the preparation of 5 infusion baggage. Fully prime infusion administration sets with admixture before inserting into the pump and connecting to the venous catheter. Patients handled with brexanolone are at threat of somnolence, excessive sedation, sudden lack of consciousness, or an altered state of consciousness throughout administration; see Dose Adjustments. Time to full restoration from loss or altered state of consciousness after dose interruption ranged from 15 to 60 minutes. There was no clear association between loss or alteration of consciousness and pattern or timing of dose. Not all sufferers who skilled a loss or alteration of consciousness reported sedation or somnolence before the episode. There was appreciable variation within the threat of suicidal ideas and behaviors amongst drugs, but an elevated danger was identified in younger sufferers for many drugs studied. Consider changing the therapeutic regimen, together with discontinuing brexanolone, in patients whose melancholy becomes worse or in sufferers who experience emergent suicidal thoughts and behaviors. It is recommended that brexanolone be tapered according to the dosage recommendations unless symptoms warrant quick discontinuation; see Usual Dose and Dose Adjustments. After signs resolve, the infusion could also be resumed on the identical fee or at a reduced fee as clinically acceptable. Patients should be accompanied throughout interactions with their child(ren) due to the potential for excessive sedation and sudden loss of consciousness. In the event of a being pregnant, enrollment in the National Pregnancy Registry for Antidepressants is encouraged. After the infusion, avoid potentially hazardous actions requiring psychological alertness, such as driving, until any sedative effects have dissipated. Request assistance throughout interactions with child(ren) due to the potential for extreme sedation and sudden loss of consciousness. Review all medicines with a health care supplier; drug interactions are attainable. Report signs of extreme sedation that will happen in the course of the infusion (patient and caregiver). Report worsening despair or the emergence of suicidal thoughts and conduct (patient and caregiver). The mostly reported adverse reactions have been dry mouth, flushing/hot flush, loss of consciousness, and sedation/somnolence. Adverse reactions leading to treatment discontinuation had been sedation-related results (loss of consciousness, presyncope, syncope, and vertigo) or infusion website pain. Adverse reactions resulting in dose reduction or interruption had been sedation-related effects (dizziness, fatigue, lack of consciousness, somnolence, syncope), adjustments in blood stress, and infusion website events. Other reported opposed occasions include diarrhea, dyspepsia, oropharyngeal ache, and tachycardia. Overdose: May result in excessive sedation, together with lack of consciousness and the potential for accompanying respiratory modifications. After signs resolve, the infusion could also be resumed on the identical or decreased rate as clinically applicable. In case of overdose, cease the infusion instantly and provoke supportive measures as essential. Recommended Dosage of Cefiderocol for Patients With CrCl Less Than 60 mL/min Estimated Creatinine Clearance (CrCl)a Dose 1. Reduced dose or prolonged intervals could also be indicated in aged patients; think about age-related impaired renal operate and concomitant illness states. No clinically important differences in pharmacokinetics of cefiderocol have been noticed based on age, sex, or race. Preparation of Cefiderocol Doses Total Volume of Cefiderocol Reconstituted Solution for Further Dilution Into at Least a hundred mL 22. The producer states that, "The compatibility of cefiderocol resolution for administration with options containing different drugs or other diluents has not been established. A cephalosporin antibacterial drug with activity in opposition to gram-negative cardio bacteria. Cefiderocol features as a siderophore and binds to extracellular free ferric iron. In addition to passive diffusion via porin channels, cefiderocol is actively transported throughout the outer cell membrane of micro organism into the periplasmic area using a siderophore iron uptake mechanism. Cefiderocol exerts bactericidal action by inhibiting cell wall biosynthesis via binding to penicillin-binding proteins. Cefiderocol has no clinically relevant in vitro exercise towards most gram-positive bacteria and anaerobic micro organism. Approval of this indication relies on restricted scientific security and efficacy information. Known historical past of extreme hypersensitivity to cefiderocol or other beta-lactam antibacterial medicine or to some other component of cefiderocol. The increase in all-cause mortality occurred in patients treated for nosocomial pneumonia, bloodstream infections, or sepsis. The safety and efficacy of cefiderocol has not been established for the therapy of nosocomial pneumonia, bloodstream infections, or sepsis. Serious and sometimes fatal hypersensitivity (anaphylactic) reactions and serious skin reactions have been reported in patients receiving beta-lactam antibacterial medication. These reactions are more probably to occur in patients with a historical past of a beta-lactam hypersensitivity and/or a history of sensitivity to multiple allergens.
|
|