|
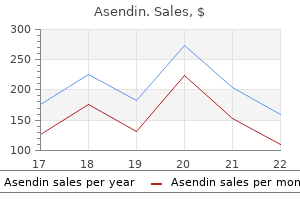
Asendin dosages: 50 mg
Asendin packs: 30 pills, 60 pills, 90 pills, 120 pills, 180 pills, 360 pills

Purchase asendin 50 mg fast deliveryWith heavy exposures depression symptoms loss of balance purchase asendin online, patients develop fever anxiety service dog order asendin from india, malaise depression general symptoms discount asendin 50mg mastercard, hepatic tenderness depression inventory order 50mg asendin free shipping, and eosinophilia,195 signs and signs that abate as the worms mature and start laying eggs within the bile ducts (Video 114. The worms elicit a fibrotic and adenomatous response in the smaller branches of the biliary ducts, which may trigger localized obstruction and hepatic abscess formation. Liver Flukes these trematodes reside in the bile ducts and are acquired by ingesting larval metacercariae encysted in freshwater fish (Clonorchis sinensis, Opisthorchis) or on freshwater vegetation (Fasciola). Most infections are asymptomatic, but these parasites could cause recurrent cholangitis. Humans purchase these parasites by ingesting metacercariae encysted on freshwater plants, corresponding to watercress. Ingested metacercariae excyst in the small intestine, penetrate via the bowel wall, and enter the peritoneal cavity, where they migrate to the liver, penetrate the capsule, and travel through the hepatic parenchyma looking for a bile duct (acute part; 2 to four months). They reside throughout the bile ducts, reaching maturity within three or four months, after which they lay eggs (chronic part; monthsindefinite). Upon reaching contemporary water, Fasciola eggs embryonate, hatch, and launch miracidia that swim in search of a suitable snail. A miracidium enters a snail and develops right into a sporocyst that asexually multiplies, ultimately releasing quite a few cercariae. The cercariae swim to a freshwater plant and encyst on the wall, awaiting ingestion by a mammal. Clinical Features and Pathophysiology Fasciola infestations often are asymptomatic. In the acute section, patients can have stomach ache and hepatomegaly because the parasites penetrate the intestinal wall and hepatic capsule. Patients additionally develop signs from migration of the parasites to other sites similar to subcutaneous fats. During the chronic phase of fascioliasis, sufferers can have symptoms of intermittent biliary obstruction and cholangitis. Visceral schistosomiasis can cause colitis and fibrosis of the portal venous system, producing portal hypertension. In most international locations by which schistosomes are endemic, some regions have a high prevalence of an infection; in other areas, the parasite appears absent. In these later areas, nonetheless, many low-level infections are missed and true prevalence is far larger than reported. It is the distribution of these snails that helps define the geographic limits of schistosomes. Construction of water reservoirs and irrigation canals has expanded the snail habitat in plenty of international locations, a follow that has increased the risk of buying schistosomiasis. Mice and different mammals also can harbor schistosomes and might allow unfold of the parasite even have been sanitation to be improved,215 thereby making schistosomiasis difficult to eradicate. Cercariae are fork-tailed, microscopic larvae that swim via the water in search of an acceptable mammalian host. Upon discovering this host, they penetrate through intact skin, shed their tails, and rework into schistosomules which are lined with a double lipid-bilayer tegument; this tegument thwarts most immunologic attacks. They migrate via the pulmonary capillaries, flow via the left facet of the center into the systemic circulation, and eventually reach the liver, the place they mature, mate, and migrate in opposition to venous circulate within the portal system. The 2-cm female is partly ensheathed by the shorter male, and the "couple" reside collectively within the mesenteric veins. The worms remain within the mesenteric vessels, consuming blood and nutrients and depositing eggs. Many of the eggs move via the intestinal wall and enter the lumen of the bowel. The eggs are excreted with the stool, and if deposited in recent water, they hatch to release ciliated miracidia. It is the distribution of snails allowing infection which determines the geographic foci of endemic schistosomiasis. For instance in Brazil, some strains of the snail Biomphalaria tenagophila are contaminated easily whereas other strains are utterly resistant. Cercariae bud off the secondary sporocysts, exit the snail, and swim in search of a permissive mammalian host. Multiple polypoid lesions because of Schistosoma mansoni are seen all through the rectosigmoid colon, which is displaced out of the pelvis by a big pericolic abscess. Patients with repeated contact can develop a mild papular rash, in distinction to the intensely pruritic papular rash that develops after exposure to avian schistosomes such as Trichobilharzia ocellata. In a suitable host, schistosomules migrate through the physique with out producing symptoms. Juvenile and grownup worms evade immune attack elegantly: Their tegument is coated with histocompatibility and blood group antigens derived from the host. Moreover, schistosomes produce a quantity of proteins that stop complement, neutrophils, macrophages, or lymphocytes from injuring them. The common life span of worms is assumed to be about 6 to 10 years, however there are documented instances of adult worms surviving for more than 35 years after persons had left an endemic area. Whereas the adult worms evade an immune response, the schistosome eggs invite one, exuding antigens that set off a powerful cell-mediated Th2 immune response. Patients have fever, malaise, arthralgia, myalgia, cough, and diarrhea, with the additional finding of marked eosinophilia. Each schistosome egg secretes antigens that provoke a focal granulomatous inflammatory response that helps move the egg from the within of a capillary, through the intestinal wall, and out into the lumen. Passage of eggs via the bowel wall causes intestinal schistosomiasis with guaiac-positive stools or even bloody diarrhea. Other eggs lodge within the mesenteric and portal veins or stay within the intestinal wall. In these places, the eggs elicit granulomatous irritation with eosinophils, macrophages, lymphocytes, fibroblasts, and mast cells. When eosinophils degranulate, they deposit main fundamental protein that produces an eosinophilic halo around the eggs, termed the Splendore-Hoeppli phenomenon. This phenomenon is nonspecific and could be seen with bacterial, fungal, and parasitic infections. Eosinophils likely assist in killing the miracidia protected by the robust egg shell. After one or 2 weeks the miracidium dies, antigen launch wanes, and the granuloma involutes to depart a fibrotic scar. Over the years, the every day production of eggs, granulomas, and scars accumulates enough harm to produce illness. Eggs that lodge in the hepatic and portal vessels produce a unique sample of scarring known as Symmers pipe stem fibrosis, during which the vessels turn into fibrotic and resemble clay pipe stems on cross part; this course of causes the pre-sinusoidal venous obstruction and portal hypertension attribute of hepatosplenic schistosomiasis (see Chapter 84). Patients typically have an enlarged left hepatic lobe, splenomegaly, and thrombocytopenia because of platelet sequestration. Hepatocellular operate remains normal as a outcome of the blood supply to the liver is maintained by increased hepatic artery circulate. Patients have normal serum aminotransferase levels with mildly elevated serum ranges of alkaline phosphatase and gamma glutamyl transpeptidase. The traditional presentation of decompensated hepatosplenic schistosomiasis is variceal hemorrhage. Hepatosplenic schistosomiasis results from accrued injury and requires extended, moderately intense infection. Patients with hepatosplenic schistosomiasis usually vary in age from adolescence to late 20s and have had schistosomiasis for 5 to 15 years. Compensated illness improves after schistosomes are killed by drug remedy, permitting the portal tributaries to heal and transform. Eggs can percolate by way of portocaval collateral vessels, lodge within the pulmonary capillaries, and over time cause pulmonary hypertension and cor pulmonale. Schistosomiasis can cause membranoproliferative glomerulonephritis or focal glomerulosclerosis with proteinuria, nephrotic syndrome, and end-stage renal disease. Schistosomal nephropathy results from deposition of immune complexes of parasite antigens and antibodies, and the renal illness could be progressive even if the parasites are killed with drug remedy.
Buy asendin 50mg on-lineProximally it receives a number of branches from the radial recurrent artery and generally a large branch from the posterior interosseous artery on the point of bifurcation into ascending and descending branches depression zoning out asendin 50mg generic. The dominant pedicles emerge from the radial recurrent artery anxiety vs stress purchase asendin cheap, entering the muscle at its proximal deep floor depression obesity discount 50 mg asendin visa. Classically this is described as emitting one or two branches to the brachioradialis and one branch each to the radial extensor of the carpus and to the supinator depression chat room asendin 50 mg cheap. The other extensor muscular tissues arise from the widespread extensor origin within the posterior compartment. They are supplied by the posterior interosseous artery, which is aided within the distal part of the forearm by the perforating terminal branch of the anterior interosseous artery. The superficial extensor muscles the anconeus muscle is a type I muscle (one vascular pedicle) according to the classification of Mathes and Nahai. Vascularisation comes from the interosseous recurrent artery, a department of the posterior interosseous artery. The posterior interosseous artery enters the posterior compartment of the forearm on the decrease margin of the supinator muscle, the place it joins the deep radial nerve. Here the posterior interosseous artery offers off the interosseous recurrent artery, which passes again beneath the anconeus muscle to the lateral elbow. It additionally gives off two or three branches to the overlying pores and skin, which passes around the lateral border of this muscle. The terminal branches of the interosseous recurrent artery anastomose on the olecranon plexus with the branches of the middle collateral artery (Anconeus flap in accordance with Cardany). The majority of the perforators are musculocutaneous and move through the flexor carpi ulnaris muscle. The radial facet of the dorsal middle and distal third of the forearm is vascularised by 4 to seven perforators from the radial artery. The majority of the perforators are musculocutaneous and cross via the brachioradialis muscle. Venous drainage can happen through the paired deep concomitant veins and thru superficial veins, radially via branches of the cephalic vein and ulnarly by way of branches of the basilic vein. Both systems are linked to one another through numerous functionally significant anastomoses. Under physiological conditions, blood flows from the deep to the superficial system upon muscle contractions within the region of the hand and forearm. In the case of distal flap stems, nonetheless, the path of blood move could additionally be sufficiently inverted owing to vascular denervation and, primarily based upon this, an increase of intravenous stress and vein architecture (cross-over pattern based on Lin and collaborators). The palmar side of the forearm is equipped by the medial and lateral cutaneous nerves of the forearm. Because of their diameter, which is approximately 2 mm, both nerves are applicable for a microsurgical nerve coaptation. Innervation of the dorsal forearm aspect is provided by the posterior interosseous nerve. These vessels may contribute to the blood provide of a radial bone element of an osteomyofasciocutaneous forearm flap. The main pedicle arises from the ulnar artery or sometimes from the anterior interosseous artery. The distal third of the muscle is provided by the interosseous artery and 3 to 4 direct branches of the ulnar artery. The anterior interosseous artery is situated on the flexor facet of the interosseous membrane and divides into its branches roughly 1 to 4 cm distally to the proximal margin of the pronator quadratus muscle. On the same top, a speaking department emerges, which anastomoses with the posterior interosseous artery via the interosseous membrane. The distal department of the anterior interosseous artery converges with branches of the palmar carpal community roughly on the height of the distal carpal row and approaches the muscle from its dorsal facet. This myoperiosteal vascular system beneath the pronator quadratus muscle additionally provides the distal portions of the radius and ulna, particularly the palmar and medial corticalis of the radius. Other than that, a further small branch off the radial artery reaches the pronator quadratus muscle from the palmar side within the majority of cases. The superficial a part of the supinator muscle is provided by the radial recurrent artery and the deep half by the posterior interosseous artery and its recurrent branch. These vessels anastomose exterior the muscular tissues in about one-third of instances, and in all cases they send a number of branches to the muscle tissue and the median and ulnar nerves. In the middle part of the forearm the superficial flexors are supplied by the ulnar and radial artery. The dominant pedicles arise from the radial recurrent artery, coming into the muscle at its proximal deep surface. The radial recurrent artery additionally supplies the extensor carpi radialis longus and brevis, the muscular branch of the radial nerve, and the pores and skin alongside the fascial septum between the brachialis and the brachioradialis. In two-thirds of instances it anastomoses with the radial collateral artery at a degree approximately three. Minor pedicles arise from the deep brachial artery between the brachioradialis and brachialis muscles and the radial artery on the forearm segment (brachioradialis muscle flap according to Ger). It is supplied by a single dominant proximal pedicle and several accent branches. Within the muscle, this artery divides into a small ascending department and a larger descending department, which anastomoses with essentially the most proximal of a sequence of 6 to eight direct small branches of the radial artery. Proximally to these, they cross the anterior floor of the pronator teres, supplying it. Its main blood provide comes from the posterior ulnar recurrent artery, which is positioned on the deep surface of the muscle close to its origin, and anastomoses with the inferior ulnar collateral artery. The anterior interosseous artery appears to be the primary periosteal and endosteal blood supply of the ulna, with its branches supplying the distal quarter of both ulna and radius. Other contributing arteries that provide the ulna include the ulnar artery, the ulnar recurrent artery and the recurrent interosseous artery. In the distal forearm the anterior interosseous artery varieties anastomoses with the radial artery, the posterior interosseous artery through the distal perforating department and the ulnar artery, forming a vascular network for the availability of the distal ulna and radius. During its course in the lateral intermuscular septum it provides off a number of periosteal branches. Innervation of the palmar forearm side is equipped by the anterior interosseous nerve. In case of a compartment syndrome of the hand there are well-defined surgical approaches to reduce the intracompartmental strain. The thumb and dorsal interosseous muscle tissue are approached dorsally via longitudinal incisions. The thenar and hypothenar compartments are approached by way of longitudinal incisions above the radial aspect of the first metacarpal and the ulnar aspect of the fifth metacarpal, respectively. The airplane of dissection is dorsal to the neurovascular bundles and anterior to the flexor sheath. Dissection is carried out across the digit to launch all parts of the compartment. The somewhat extra advanced architecture of the palmar side of the hand leads to a topographical structuring into three areas. Likewise, the palmar side of the fingers permits a topographical separation in two layers solely, particularly a superficial subcutaneous or epivaginal and a deep subtendinous layer, which refers to the space between the vagina fibrosa and the phalanges. Besides this horizontal structuring, the palm of the hand beneath the aponeurosis and the fascia which it emits laterally could be split up in lateral compartments. Besides several smaller cutaneous branches of the again of the hand, it frequently divides into four to five dorsal digital nerves, which course to the two dorsal side margins of the first two fingers and to the radial margin of the center finger. An anastomosis to the dorsal department of the ulnar nerve is established within the distal area of the back of the hand by way of the communicating ulnar department. Besides the connecting branch to branches of the radial nerve it develops three to five dorsal digital nerves, which method the marginal edges of the fourth and fifth fingers and supply these up to and including the median phalanges. The distal phalanges of the first three fingers and part of the distal phalanx of the fourth finger are innervated palmarly via the right palmar digital nerves of the median nerve. The median sector of the dorsal circumference of the wrist is then reached by the distal branches of the posterior cutaneous nerve of the forearm, which emerge from the deep branch of the radial nerve. Among the several variants of the cutaneous branches of the radial and ulnar nerves described in literature the attainable absence of certain stems ought to be talked about here. For occasion, elements of the region in any other case innervated by the dorsal branch of the ulnar nerve may be equipped by the superficial department of the radial nerve.
Buy asendin usThe motor department for the extensor carpi ulnaris muscle might course above or below the interosseous artery and should be spared if displayed during the preparation of the artery mood disorder screening tool order genuine asendin on-line. After emitting its motor branches depression symptoms more common in adults purchase asendin 50mg with amex, the delicate distal branch of the deep department of the radial nerve depression japan purchase asendin online, the posterior interosseous nerve bipolar depression episode order cheap asendin on-line, programs beneath the proper extensor indicis muscle on the interosseous membrane to the dorsal wrist capsule. It tasks onto the connecting line between the lateral epicondyle of the humerus and the distal radioulnar joint, on whose central third, i. After outlining the flap borders, preparation begins within the distal third of the forearm with a small incision within the area of the distal radioulnar joint for identification of the distal anastomosis of the posterior and anterior interosseous artery. The intermuscular septum is found by identification of the septal arteries, which run via the deep fascia into the skin. The tendons of the extensor digitorum and extensor indicis muscle tissue are retracted radially. Fixing pores and skin and fascia with a few stitches is adopted by radial preparation as a lot as the intermuscular septum, which may not be severed, though, to find a way to save at least the thickest proximal vessel with its irradiation of the distal skin portion. The deep source arcade of the extensor digitorum muscle ought to be incised to enable an excellent view of the artery the place it emerges beneath the supinator. Proximally, the artery should be ready from the deep department of the radial nerve, which is situated laterally, with the help of magnifying glasses. It then passes through the interosseous membrane, between the proximal and distal third about 6 to 8 cm distal to the epicondylus lateralis humeri and attains the posterior compartment of the decrease arm beneath the supinator muscle. There it courses in a septum-like tumescence of connecting tissue on the interosseous membrane to the distal side, emits several branches to muscles, bones and skin and anastomoses with the dorsal carpal network. In its proximal third, the posterior interosseous artery passes between the abductor pollicis longus muscle and the extensores digiti minimi or carpi ulnaris muscle tissue, which it supplies by way of brief muscle branches. Musculoperiosteal branches also course to the extensores pollicis longus and indicis proprius muscular tissues and the medial aspect of the ulna. In the middle third of the lower arm, the posterior interosseous artery lies, very near to the floor, beneath the forearm fascia in an intermuscular septum between the extensor digiti minimi muscle (on the radial side) and the extensor carpi ulnaris muscle (on the ulnar side), which it supplies via quite a few small muscle and tendon branches. In these circumstances the center section is related to the anterior interosseous artery through a strong perforating branch. In its distal third the posterior interosseous artery provides the median edge of the radius via direct periosteal vessels. Immediately proximal to the distal radioulnar joint, near the metaphysis of the ulna, it anastomoses with the anterior interosseous artery through the communicat- 5. Occasionally, the motor department to the extensor carpi ulnaris muscle crosses above the artery, which should then be ligatured distally to this essential motor nerve. After fixing skin and fascia with a few stiches, the intermuscular septum is uncovered from the ulnar aspect by retracting the extensor carpi ulnaris muscle and its tendon. After release of the tourniquet, retrograde perfusion is checked and a whole haemostasis obtained. Finally the intermuscular septum is separated sharply, from proximal to distal, from the ulna to the distal vessel anastomosis, which signifies the rotation level. Afterwards, an intensive course of physical therapy as nicely as scar and pores and skin transplant treatment must be offered. Due to the long and conspicuous scar on the forearm this flap must be used with ladies (for the same indication) only when a radial artery flap would result in a functionally and aesthetically worse result because of a thick subcutaneous layer. Further indications for the posterior interosseous artery flap are defects of the gentle elements in the area of the dorsum of the hand. Because of the somewhat quick dorsal vessel pedicle, defects within the delicate components of the palm can only be coated reliably in the proximal hypothenar and thenar areas without having to take into account an unfavourable relaxed position in hyperextension. The pure fascia flap is suitable for the reconstruction of the portions within the area of the wrist and back of the hand and together with a medium split-thickness pores and skin graft and likewise for the reconstruction of the skin defects in this area. On account of the difficult vascularisation the posterior interosseous flap is contraindicated in emergency conditions and with pre-existing accidents within the distal forearm and wrist areas. Now the skin is prepared on both sides with some subcutaneous tissue to forestall injury to the subdermal vessel plexus. Selected readings Osteo-myofascicutaneous posterior interosseous artery composite flap A muscle sleeve containing the musculoperiosteal department of the posterior interosseous artery could be raised from the extensor pollicis longus muscle along the attachment to the intermuscular septum along with a 8- by 5-cm vascularised bone transplant from the mediodorsal ulna. The anterior interosseous artery reaches the house between the palmar bones after it has coursed through or underneath the pronator teres muscle together with the stem of the median nerve. With short lateral branches it innervates the flexores pollicis longus and digitorum profundus muscles and then, with its long terminal department, the pronator quadratus muscle. The fasciocutaneous flap is centred on the projection line of the anterior interosseous artery between the dorsal tubercle of the radius (Lister) and the lateral limits of the elbow crease, at concerning the height of the upper perforating branch. A skin area from the proximal wrist crease to the proximal third of the forearm could be raised, if required. The upper perforating branch of the anterior interosseous artery is identified by slight traction on the extensor pollicis muscle in its course on the inside side of the extensor pollicis brevis muscle. Subsequently its muscle branches are ligatured, the intrerosseous membrane is incised and the now revealed anterior interosseous artery is ready to distal. In order to lengthen the vessel pedicle, the palmar terminal department of the anterior interosseous artery, as well as the distal anastomoses, can be ligatured to the posterior interosseous artery, whereas the anterior interosseous artery itself remains intact. After launch of the tourniquet, the circulation of the anterior interosseous artery proximal to the exit of the superior perforating branch is interrupted with a microclamp and the retrograde perfusion of the flap is checked. Twisting of the vascular pedicle during flap transposition have to be strictly averted. This ought to be followed by intensive physical remedy in addition to care of the skin transplant. Selected readings: 5 Surgical anatomy the anterior interosseous artery emerges from the short stem of the widespread interosseous artery, passes by way of the deep head of the pronator teres muscle and courses to distal on the interosseous membrane. It supplies all muscular tissues of the deep palmar layer through muscle branches and by way of the 2 nutrient arteries to the radius and ulna. In the median and distal areas the anterior interosseous artery shares in the provide of the dorsal aspect of the forearm. Usually, there are two anastomoses with branches of the posterior interosseous artery, which can emerge from the anterior interosseous artery either separately or jointly. After penetrating the interosseous membrane it involves lie in a septum-like thickening of connective tissue between extensor indicis and extensor pollicis longus muscles (on the ulnar side) or, correspondingly, within the extensor pollicis brevis muscle (on the radial side) to which it emits branches. The metaphysis and diaphysis of the distal dorsoradial facet of the radius is provided by way of three to 5 periosteal vessel branches. The distal branch extends to a skin area of about 10 by 14 cm in the median and distal thirds of the dorsal forearm. The distal (inferior) perforating department lies four to 5 cm proximal to the radiocarpal joint. From right here, too, branches emerge to the skin, muscles and bones on the distal dorsoradial radius surface. A pure fascia flap is appropriate for the reconstruction of the paratenon tissue of the wrist and dorsum of the hand. The osteo-fasciocutaneous flap is indicated for reconstructing smaller bone defects within the area of the wrist, metacarpus and thumb. Because of the shut relationship between the primary vascular supply and the underlying bone, this flap is contraindicated in emergency conditions with pre-existing injuries within the distal forearm and wrist areas. A layer of subcutaneous tissue of approximate thickness should remain on the thin forearm fascia to avoid injury to the native capillary network. The further operative and postoperative procedures correspond to these described for the fasciocutaneous flap. Selected readings Indications and contraindications the fasciocutaneous anterior interosseous artery flap is appropriate for secondary reconstruction of skin defects of the dorsum of the hand as far as the basal phalanx, of the first commissure, and, with limitations, the palm Hu W. The paraneural vessels vascularise the vein walls, forming a small longitudinal vascular arcade along the veins. The basilic and cephalic veins and the accompanying cutaneous nerve keep a detailed relationship with the neurocutaneous perforators. Both skin and nerves are vascularised by neurocutaneous perforators that stem from the major vessels of the forearm. Thus, the distal neurocutaneous perforators are of nice importance for the distally based mostly neurocutaneous flaps. Alongside the arterial paraneural vessels, two small veins could be found to drain into the deep venous system and not instantly into the basilic or cephalic vein.
Order asendin 50 mg visaAfter flap transposition depression symptoms up and down purchase asendin once a day, the center limb of the suture line extends precisely vertically within the direction of the center limb of the original Z-slice depression definition weather asendin 50 mg sale. For the incision of the skin flap mood disorder group curriculum generic asendin 50 mg on-line, the cuts should be perpendicular to the surface of the pores and skin so that a thicker flap is attained with good circulation depression easy definition cheap asendin 50mg online. Both pores and skin flaps are separated from the underlying tissue and subsequently reciprocally exchanged. After release of the tourniquet, the circulation of the flap is managed and a meticulous haemostasis is carried out. Postoperatively, the hand is immobilised for 10 to 14 days on a palmar, below-elbow splint. After resolving the flexion contraction, physiotherapeutic treatment must be supplied so as to forestall contracture recurrence. However, the longer the middle limb of the Z-incision is, the longer the two lateral incisions of the 2 lateral incisions should be. However, this is solely potential when the amount of skin needed for the skin flap is out there on each side of the wound. Altogether, the identical elongation is achieved that would have been attained with a single, largely elongated Z-plasty. On one finger, so many Z-plasties can typically be carried out constantly as phalanges are current. Should the scar cross a flexor fold, the lateral limb of the Z-plasty should be cut so that it ends on the mediolateral endpoint of the fold. In this manner, the transverse suture line may be positioned instantly into the flexor fold after transposition, while it may be essential to elongate the longitudinal incision. Since the finger becomes narrower towards the fingernail, the flap for the Z-plasty continues to slim in a distal path. There is one prerequisite to an environment friendly extension in the affected space of pores and skin: the extension resulting in the one path could be compensated by a shortening within the other course. Corrections in the space of the distal to the interdigital creases can also be carried out beneath local anaesthesia and a tourniquet utilized to the bottom of the finger. According to Limberg, the elongation impact with the easy two-flap Z-plasty depends on the angles of the triangles. With an rising angle, the flap transposition becomes more difficult, which leads to increasing pressure during closure. Transposition, though, results in a closely V-shaped and slim dorsal commissural plate In general, a four-fold Z-plasty ought to be employed to find a way to broaden the interdigital folds, since this results in a commissure with well-curved margins. Indications and contraindications Simple two-flap Z-plasty is indicated as the only steady, multiple Z-plasty or multiple-flap Z-plasty procedure for assuaging linear adhesions with none bigger defect remnants (bridging) within the area of the palm of the hand, the dorsum of the hand, the palmar aspect of the fingers and primarily in the interdigital finger folds. Through the trade of the skin flaps, the contracture is interrupted and the danger of recurrent contracture is decreased considerably. Note flap the observe flap is a triangular transposition flap designed to shut small spherical defects. The tip of this flap can be de-epithialised or trimmed when the flap is inset into the defect. In step one, the skin surrounding the defect is undermined, then the primary of the triangular skin flaps is incised and ready, and transposed into the defect in an opposing path. In this fashion, a achieve in floor space is achieved in the course of the bottom of the triangles, whereas their dimensions within the perpendicular path turn into smaller. After release of the tourniquet, the circulation of the flap is assessed and meticulous haemostasis is carried out. After a drain has been inserted, all 4 skin flaps are sutured in place without tension. The hand is immobilised in a lower-arm palmar splint in an intrinsicplus position for 10 to 14 days till wound therapeutic is full. Along the outer margin of the first flap, the outer margin of the second, larger skin flap is marked. After release of the tourniquet, the perfusion of the pores and skin flap is assessed and a meticulous haemostasis is carried out. Intensive physiotherapeutic exercises in addition to pores and skin and scar care should be initiated after about 14 days. This can be the case for circular defects after their transformation into rhomboid or hexagonal form, making simultaneous use of two, three or extra flap plasties. The first is an extension of the shorter diagonal of the rhomboid defect, and the second line is an extension of the margin of the defect. Depending on the selection of the defect margin as a margin of the flap, 4 different incisions are attainable. Prior to the skin incision, the potential of a tension-free closure of the elevation defect in the rhomboid flap ought to be checked with the so-called pinch check. The pores and skin flaps are incised and ready along with the subcutaneous the technique in accordance with Dufourmentel makes use of a modification of the incision to attain a broader base of the flap than that discovered in the authentic technique in accordance with Limberg in order that it leads to extra reliable circulation in the region of the tip of the flap. To close a whole defect of the axillary subunit, the primary choice remedy is the rhomboid flap in accordance with Limberg or Dufourmentel. Mathematical principles of local cosmetic surgery procedures on the surface of the human body (Russian). At the ends of the flap, the incision is extended in a straight line by 2 to four cm. After dissecting the veins within the area of the straight incisions, the skin across the flap is incised. Flap preparation is carried out within the layer between the subcutis and the fascia or the peritendineum, leaving the venous flap connected to the donor website both proximally and distally by method of veins. After bilateral ligature and marking of the distal finish of the flap, the flap is eliminated, and the direction of the blood circulate is marked. The donor web site defect on the foot, the dorsum of the hand or upper arm can often be closed primarily after blunt undermining of the wound margins. Taking into consideration the course of the blood circulate, as decided by the valves, the venous flap is reversed and sutured into the recipient site. Generally, two to three anastomoses are required each proximally and distally in order achieve a move by way of the flap. After full haemostasis, the margin of the flap can easily be sutured into the defect. The hand is postoperatively immobilised in a thick cotton-wool replantation dressing for five days. After this microvascular intervention, a concomitant steady management of the circulation in the pores and skin flap is recommended. Postoperatively, venous flaps undergo very attribute stages: Intraoperatively and on the 1st postoperative day, they normally demonstrate a rosy or solely slightly bluish complexion. In the occasion of in depth cyanosis and beginning epithelial desquamation, one ought to consider scarification and hourly use of heparin soaked gauzes or, alternatively, the application of leeches. The blood flow in the venous flap is retrograde from the vein by means of a venule into the capillaries and as soon as once more right into a vein. The retrograde circulate of blood could be assessed clinically using the time to recapillarisation of the skin flap or a venogram. After a heat bathtub and software of a tourniquet, the world with the densest venous plexus can already be marked preoperatively, the place the number of the donor site is topic to aesthetical and useful aspects. Taking the subcutaneous venous plexus into consideration, an space of the pores and skin may be marked with a maximum of 5 cm in size and three cm in width. The position of the various possibilities for the connection, for the nourishment and fee of mortality of the transplant, however, has not been totally clarified but. Venous flaps can be vascularised from proximal, additionally by the use of orthograde blood circulate, or from distal by means of retrograde blood flow. Indications and contraindications Free microvascular venous flaps have maximal dimensions of 4 to 10 cm2. The purely venous fascia flap plasty is suitable for overlaying defects associated with circular avulsion accidents. Because of the excessive rate of failure with larger flap dimensions, the Selected readings Carrel A, Guthrie C. The descending branch passes downward into the intermuscular septum between the rectus femoris muscle and the vastus lateralis muscle. The descending branch often divides right into a lateral descending department and an innominate medial descending department. The medial branch programs distally posterior to the rectus femoris muscle and is often smaller than the lateral department.
Order asendin discountIn vitro assays proved particularly helpful in demonstrating direct results on tumor cells similar to apoptosis induction depression test learnmyself purchase asendin american express, inhibition or stimulation of cell signaling depression symptoms body pain purchase asendin 50 mg with amex, blockade of progress components anxiety 1st trimester purchase asendin paypal, and cell proliferation anxiety treatment natural 50mg asendin otc. Antibodies mediate completely different effector features through distinct domains of the antibody molecule. Several lines of evidence help the function of Fc-mediated effector functions for the efficacy of antibodies in animal models. Probably the most direct proof for individual effector mechanisms is derived from genetically modified mice. However, more recent studies demonstrated that antibodies towards different target antigens. Thus, choice of the tumor target antigen decided the engagement of optimum Fc receptors in mice, and thereby the choice of the most appropriate antibody isotype [17]. However, mouse and human antibody isotypes in addition to their respective Fc receptors share solely restricted homologies, and the mobile expression patterns of the various Fc receptor isoforms are significantly different [18]. Thus, for human IgG1 antibodies the in vitro activity with human complement and human effector cells correlated reasonably nicely with their in vivo exercise in mice, while these correlations have been less obvious for different human IgG isotypes [19]. Additional complexity was demonstrated in studies suggesting that different effector mechanisms of rituximab prevail at different anatomical sites [23]. Furthermore, antibody concentrations affected the contribution of various effector mechanisms as direct growth inhibition was more relevant at saturating concentrations, whereas Fc receptor-mediated killing predominated at decrease antibody doses [8, 24]. Induction of tumor-directed immune responses after antibody therapy have repeatedly been reported in animal models. Furthermore, response to rituximab correlated with the expression of sure Fc receptor alloforms. In addition to supporting the position of Fc receptormediated MoA, these research additionally counsel particular effector cell populations to be clinically relevant. Although proof for systemic complement activation after rituximab therapy has been noticed in a number of studies [40], its contribution to the killing of lymphoma cells in vivo is more controversial. Since systemic complement activation after rituximab utility might play a key position for the side effects of this remedy [43], potential advantages of modified antibody constructs with increased capability to activate the complement need to be balanced against the danger of more severe toxicity. So far, the clinically relevant MoA for therapeutic antibodies towards strong tumors are even more elusive. Here, out there data suggests a stronger impression of tumor cell-related factors somewhat than antibody-mediated functions [45]. Also in stable tumors the influence of individual effector mechanisms could rely upon the medical state of affairs, because the efficacy of trastuzumab within the adjuvant setting was not correlated to the established Fc receptor polymorphisms [49]. In this section, we focus on the rationale for utilizing this isotype, and discuss potential alternate options, the number of which is dependent upon the required effector capabilities and on pharmacokinetic traits. Recently, subclass-dependent variations within the affinities for particular activating or inhibitory murine Fc receptors were described. The ratio of activation to inhibition (A/I ratio) differed by a quantity of orders of magnitude between the murine IgG subclasses, and predicted the in vivo exercise of antibodies in two different models [13]. Also within the human system, four IgG subclasses (IgG1, IgG2, IgG3, and IgG4) have been distinguished serologically [51] and genetically [52]. In man, average serum retention half-life of 21 days has been reported for IgG1, IgG2, and IgG4 antibodies, whereas IgG3 antibodies have a half-life of solely 7 days [53] (Table 7. However, the lower half-life of IgG3 antibodies may be overcome by using a particular IgG3 allotype (H435 vs R435), displaying related FcRn binding characteristics as human IgG1 [54]. Furthermore, human IgG subclasses additionally display differential specificities and affinities to activating and inhibitory FcR (Table 7. Further variation within the human -heavy-chain genes and subsequent heterogeneity within the IgG proteins have been described, collectively called the Gm allotype system. The practical relevance of these allotypes is broadly unclear, however a minimal of two IgG3 allotypes had been reported to differ in their capability to activate the complement system [57, 58]. This area also contains the binding websites for complement C1q and Fc receptors, and determines the flexibility of the molecule [59] (Table 7. The preliminary event in the activation of the classical complement pathway is fixation of C1q within the vicinity to the cell floor by the Fc parts of at least two antibodies. The capacities of the four human IgG subclasses to bind C1q have been determined utilizing matched units of chimeric antibodies with equivalent variable areas [57]. Furthermore, IgG1 proved to be the best subclass at excessive antigen densities. IgG3 was superior at decrease antigen concentrations owing to its higher flexibility and longer hinge region, which collectively provide the potential to span longer distances between target antigens expressed on the cell surface [62Ͷ4]. Interestingly, IgG2 was demonstrated to mediate effective complement lysis at very high antigen densities by additional activation of the choice pathway, which is regarded to be especially necessary for opsonization and killing of bacteria [62]. Antibodies interact with effector cells through binding of their Fc area to cellular Fc receptors [60, 65]. This course of leads to both activation or inhibition of effector cells, relying on which Fc receptors are predominantly engaged. Human FcRs have been demonstrated to comprise differential IgG subclass specificities (Table 7. On the other hand, human IgG3 has been advised to be a stronger molecule at lower target antigen expression levels, while human IgG4 appeares to be a candidate isotype, if interactions with the host immune system are undesired. However, IgG4 antibodies generally tend to type half-molecules, which can be exchanged between two IgG4 molecules [67Ͷ9]. This instability of human IgG4 could be corrected by a single S228P mutation within the hinge region [70]. For therapeutic purposes, IgG4 molecules have been additional engineered by E235S mutation, leading to full incapacity to work together with cellular Fc receptors [71]. Two isotypes IgA1 and IgA2 are distinguished, with IgA2 having a shorter hinge region and an increased resistance against enzymatic degradation by bacterial proteases. After covalent binding to the joining (J)-chain, both IgA isotypes type dimeric IgA, which binds to the polymeric immunoglobulin receptor (pIgR) to generate secretory IgA after transepithelial transport and luminal proteolytic cleavage [75]. IgA antibodies effectively activate human myeloid cells (neutrophils, monocytes, and macrophages), which constitute the first-line cellular protection towards micro organism and fungi. Furthermore, myeloid cells can kill a broad spectrum of tumor cells and are critically involved in tumor rejection in animal models [77, 78]. Especially neutrophils, the most numerous phagocytic cell population in vivo, are activated extra effectively by IgA than by IgG1 antibodies [79, 80]. However, totally different stoichiometric interactions with Fc receptors, inside-out signaling, as nicely as more intense interactions with the widespread FcR chain might explain the enhanced activation of myeloid effector cells by IgA in comparability with IgG antibodies [83]. Furthermore, pharmacokinetic properties of IgA are essentially different from those of IgG as dimeric IgA is actively transported onto mucosal surfaces, and IgG however not IgA binds to FcRn and is due to this fact shielded from degradation and clearance [84]. With regard to therapeutic functions, molecules of the IgA2 isotype display a quantity of advantages compared to molecules of IgA1 isotype. Additional challenges in phrases of antibody production and high quality control are posed by the O-glycosylation positioned within the hinge region of IgA1 antibodies. Furthermore, naturally occurring alterations on this O-glycosylation had been demonstrated to be critically involved in the pathogenesis of IgA nephritis a typical and sometimes critical form of glomerulonephritis associated with IgA-containing immune complexes [85]. The IgA2 m(1) alloform is most typical in Caucasians, however accommodates an unusual, noncovalent heavy- and light-chain linkage, which may be transformed to the standard covalent heavylight chain pairing by introducing a single P221R amino acid change in the heavy chain [86, 87]. Additional modifications might further enhance the traits of monomeric IgA antibodies as therapeutic molecules. In vitro, dimeric IgA proved simpler than monomeric IgA antibodies, which is probably defined by their larger valency for both goal antigen and Fc receptor binding [88]. In vivo, intravenously applied dimeric IgA, which is directionally transported via epithelial cells by way of pIgR, might goal pathogens or widespread tumors corresponding to lung or colon cancers from the luminal floor, which under pathologic conditions accommodates elevated numbers of neutrophilic effector cells. Earlier research demonstrated therapeutic results of IgA antibodies in infectious diseases [90, 91]. Since the activation of leukocyte Fc receptors depended on Fc glycosylation, it was supposed that the oligosaccharide moiety exerted its influence not directly in all probability through modulation of the Fc conformation [98ͱ00]. Interestingly, recent information from co-crystal structures of Fc variants and glycosylated FcR variants suggested that carbohydrateΣarbohydrate interactions between Fc- and FcR-bound glycan constructions are also crucial for the affinity of FcR binding [102, 103]. From these observations, two approaches to modulate Fc functions turned evident: altering the glycosylation profile (see Chapter 8) or mutation of selected amino acids in the IgG Fc portion (protein engineering). Decreased Fc receptor binding seems significantly engaging for immunoconjugates, however naked antibodies have additionally been developed that should not bind to leukocyte Fc receptors. Diminished Interactions with Fc Receptors For antibodies that should not bind to mobile Fc receptors, F(ab)2 fragments can be a logical step ahead, but F(ab)2 fragments are expensive to produce and have a brief plasma half-life as a end result of their lack of binding to FcRn. Therefore, whole IgG antibodies have been engineered that display reduced affinity in Fc receptor binding.
Order asendin cheapPrevalence and medical significance of intestinal microsporidiosis in human immunodeficiency virus�infected patients with and without diarrhea in Germany: a prospective coprodiagnostic research depression symptoms female buy discount asendin 50 mg on-line. Entercytozoon bieneusi an infection in an immunocompetent patient who had acute diarrhea and who was not contaminated with the human immunodeficiency virus depression quotes buy asendin 50mg otc. Molecular phylogeny of the microsporidia: ecological depression worse in morning buy asendin without a prescription, ultrastructural and taxonomic concerns depression retreat cheap 50mg asendin otc. Polymerase chain reaction detection of Trypanosoma cruzi in human blood samples as a device for analysis and remedy evaluation. Short report: comparison of the results of sublingual nifedipine and isosorbide dinitrate on oesophageal emptying in patients with chagasic achalasia. Modern travel, emigration,1,2 and consumption of "exotic" cuisines permit intestinal helminths to appear in any locale. People now acquire tropical helminths without leaving their industrialized temperate cities. Because intestinal helminth infections are extra frequent in developing international locations, full journey historical past is a critical-but usually overlooked-aspect of the patient interview. Helminths may survive for decades inside a host, so even a distant historical past of visits to or emigration from nations where helminths are endemic is important. Fresh meals is flown all over the world and infrequently consumed raw, usually at a great distance from its authentic level of origin. Physicians must remain alert to the potential for infection with these organisms as a outcome of some trigger extreme disease that requires years to develop or happens only under special circumstances. For instance, sufferers might have occult Strongyloides stercoralis until remedy with glucocorticoids causes fulminant disease, occult Clonorchis sinensis till they develop cholangiocarcinoma, or occult Schistosoma mansoni until they develop portal hypertension and bleeding from esophageal varices. In developed international locations, intestinal helminths usually are identified as an sudden discovering rather than because of an actively pursued diagnostic evaluation. Helminths are complex organisms well-adapted to their hosts; like quiet house visitors, most trigger no symptoms. Physicians must talk their concerns of attainable helminthic an infection to laboratory personnel. A telephone call to the native laboratory earlier than a pattern is distributed can improve diagnostic results dramatically. Occasionally, alarmed sufferers deliver proglottids or entire worms that they passed with their stools. These specimens must be mounted in 5% aqueous formalin and despatched for identification. Some helminthic infections are difficult to diagnose, particularly when the worm burden is gentle. It is even attainable that exposure to helminths affords some protection towards illness as a end result of sturdy immune reactions. Helminth associated safety from pathogenic inflammation may be mediated, a minimum of in part, by modifications within the microbiome. Several potential mechanisms have been proposed to clarify how helminths alter the composition of microbiota. Bacterial attachment (a key set off of colitis) was reduced after Trichuris publicity. In addition, helminth merchandise also can directly influence cell responses in animal models of metabolic syndrome. Fertilized eggs are handed in stool and incubate within the soil for 10 to 15 days whereas the embryo develops and molts twice, after which the eggs turn into infective. The eggs are remarkably stable, can survive freezing, and might remain viable for 7 to 10 years. The eggs are resistant to most chemical treatments together with pickling, however they quickly die in boiling water. Once ingested, eggs hatch within the duodenum and launch their larvae, which penetrate the intestinal wall and enter the mesenteric venules and lymphatics. Larvae that migrate with portal blood pass to the liver, by way of the sinusoids to the hepatic veins, after which by way of the proper facet of the heart to enter the lungs. Larvae migrating by way of the lymphatics move via mesenteric lymph nodes to the thoracic duct and enter the superior vena cava, also to arrive within the lungs. The larvae then lodge in the pulmonary capillaries and break into the alveoli, where they molt twice while rising to 1. Larvae then ascend the tracheobronchial tree, arrive within the hypopharynx, are once more swallowed, and move into the small intestine, where they molt again and eventually mature. The pneumonitis often is self-limited but could be life-threatening if larvae are numerous. Large numbers of mature worms can cause severe intestinal signs including stomach ache, distention, nausea, and vomiting. Fatality results from intestinal necrosis attributable to obstruction, intussusception, or volvulus. Fertilized eggs are 35 by 55 m and have a thick shell and outer layer; females additionally lay unfertilized eggs which are larger (90 by 44 m) and have a skinny shell and outer layer. Disease normally develops solely in these with heavy worm burdens: pulmonary, intestinal, and hepatobiliary ascariasis are well-described. Pulmonary ascariasis (Ascaris pneumonitis) develops 4 to sixteen days after ingesting infective eggs. Albendazole is poorly absorbed but continues to be thought of possibly teratogenic, and when attainable, therapy with this agent ought to be delayed till after delivery. Previously, clinicians who work in endemic countries would keep away from treatment of pregnant women, nonetheless, in areas the place repeated pregnancy is widespread, this resulted in prolonged avoidance of probably life-saving therapy. A recent research of 1257 girls handled with albendazole showed no opposed effect of albendazole remedy on delivery weight, perinatal mortality, or congenital anomaly in contrast with placebo. The first dose kills mature worms which have completed their migration to the intestine, and the second dose kills worms that were in transit when the primary dose was given. Albendazole is properly tolerated, but can cause nausea, vomiting, and stomach pain. Albendazole may be held until after the obstruction has resolved and then is used to eradicate any remaining organisms. Hepatobiliary ascariasis also may be treated conservatively with fluid resuscitation, bowel relaxation, and antibiotics. This feature of albendazole is advantageous because were paralyzed worms inside the duct unable to move out via the sphincter of Oddi, they might turn out to be trapped within the bile duct. Patients with hepatobiliary ascariasis must be treated with albendazole every day for several days as a end result of the worms solely turn out to be susceptible to the drug after they migrate out of the bile duct. Worms can also invade the pancreatic duct and intrapancreatic Ascaris can be treated just as hepatobiliary ascariasis. Ampullary sphincterotomy permits worms simpler access to the ducts and can improve the danger of recurrent pancreaticobiliary ascariasis. Filariform larvae develop throughout the gut, migrate alongside outlined paths, and mature to increase the variety of adult parasites in the host; this ends in extended an infection that may extend to 75 years, after one leaves an endemic space. Immunosuppression or glucocorticoid administration upsets this stability with the end result that previously asymptomatic, but chronically infested, sufferers develop fulminant, potentially fatal strongyloidiasis from huge autoinfection. In addition, glucocorticoids can act instantly on the parasites to increase the development of infective filariform larvae. Migrating filariform larvae injure the intestinal mucosa and carry luminal bacteria into the bloodstream, resulting in polymicrobial sepsis with enteric organisms; Streptococcus gallolyticus (previously S. Numerous larvae migrating through the lungs cause pneumonitis, and worms can arrive in uncommon locations such because the brain. Patients from endemic areas, navy veterans who served in Asia, and prisoners of warfare are at excessive risk for subclinical strongyloidiasis. Because chronic strongyloidiasis can stay subclinical and difficult to detect for many years, nevertheless, therapy of seropositive patients is warranted. A 10-fold more sensitive approach is to spread stool on an agar plate and look for serpentine tracks left by migrating larvae. Rhabditiform larvae develop within the soil into mature adults to full the life cycle of this worm. Rhabditiform larvae (250 m) can also become longer (500 m) infective filariform larvae that may penetrate any space of skin that contacts soil, after which they migrate by way of the dermis to enter the cutaneous vasculature. The larvae circulate with the venous blood until they attain the lungs, the place they break into the alveoli and ascend the bronchial tree. The worms then are swallowed with bronchial secretions and move into the small intestine, the place they embed in the jejunal mucosa and mature.
Diseases - Ventricular fibrillation, idiopathic
- Hand foot uterus syndrome
- Thrombocytopenia chromosome breakage
- Langerhans cell granulomatosis
- Rod monochromacy
- Retinitis pigmentosa
- Preeyasombat Viravithya syndrome
- Sweatalitus disease
- Chromosome 7, monosomy 7q21
- Blue cone monochromatism
Order asendin ukThe thickness of the free microvascular muscle flap leads to depression definition nice purchase asendin line (temporary) limitations depression symptoms francais cheap asendin american express. Following secondary atrophy of the denervated muscular tissues depression risk factors asendin 50mg low price, a suitable contour of the palm can be achieved depression job burnout order 50 mg asendin with visa. If the scale of the defects permits, however, the axially pedicled groin flap according to McGregor or the abdominal skin flap according to Zoltan should be most well-liked. Aside from the disadvantages arising from long immobilisation (minimum of three weeks) both flaps lead to in depth cutaneous instability because of the thick subcutaneous tissues. Aside from the laterodigital transpositional flap in accordance with Bunnell, the dorsal flag flap based on Vilain or its variants, the seagull flap variant in addition to the lateral island flap in accordance with Rose are appropriate as well. Due to the need for early mobilisation, microvascular flaps have to be most well-liked over pedicled flaps and distant flaps because care is simpler and the psychological impression on the patient is reduced. The free mobility within the region of the first commissure is a prerequisite for the oppositional movement of the 1st ray. A restriction results in a major limitation within the power-grip, key-grip and pinch-grip functions of the wholesome hand. Successful release of the constructions (so-called crescendo of the commissurolysis) may be essential for the re-establishment of the movement amplitudes. The 1st commissure begins comparatively far proximally on the tip of the first interdigital area. Due to this inclination, the extensor aspect of the thumb appears to be round 2 to three cm longer than the flexor facet. As seen from the ends of the fingers, the dorsal floor reveals a light indentation. The adducted thumb has pores and skin pulp on the radial aspect of the hole of the hand, which dorsally conforms to a prolonged prominence fashioned by the first dorsal interosseous muscle. If the thumb is brought into an kidnapped place, the skin fold, which bridges the adductor pollicis and 1st dorsal interosseous muscle tissue, turns into tense. In palmar (abduction) opposition, the oblique fold from the palmar aspect of the 2nd metacarpal head to the palmar facet of the head of the proximal phalanx of the thumb turns into tense. According to Zoltan, the first commissure consists of two triangular plates that are positioned on the tip and meet on the margin of these folds. To stop postoperative limitations in mobility and extreme scar formation via secondary contractures, some elements must be taken into consideration. In the region of the commissure, the intersection of a pores and skin transplant or the margins of a flap proceed alongside the anatomical folds or parallel to them. A parallel incision to the margin of the distal commissure have to be prevented because of the chance of tension-related hypertrophic scar formation. Near or distant flap should be sutured in place with maximal spreading of the commissure. Since the skin defect in the region of the commissures is underestimated, an excessive correction should be tried primarily. Due to secondary scar contractures, secondary wound therapeutic in the area of the commissures should be prevented. The alternative of the process for reconstructing a commissure is determined by the localisation and dimension of the skin defects. In the presence of accidents or scarring of the 1st commissure, one should examine precisely whether the defect only extends to the edge of the fold and to what extent the fold of the commissural plate has shrunk or is missing, as, for instance, is the case with congenital syndactyly. Clinical expertise regarding the therapy has shown that the following classification has confirmed useful: We can differentiate between a linear scar within the region of the distal margin of the fold, multidimensional defects within the region of the distal commissural edge and the dorsal commissural plate, multidimensional defects in the region of the distal commissural margin and the palmar commissural plate, defects on each commissural plates of the interdigital fold (syndactyly), multidimensional defects of the distal commissural margin and the dorsal commissural plate in combination with extensive defects on the dorsum of the hand and proximal carpometacarpal articulation of the thumb and, finally, multidimensional defects of the distal commissural margin and the palmar commissural plate in combination with intensive palmar and proximal defects on the carpometacarpal articulation of the thumb. Since solely a V-shaped interdigital fold reconstruction can usually be carried out with a two-flap Z-plasty, the four-flap Z-plasty according to Woolf and Broadbent ought to preferably be chosen. The two-flap Z-plasty is preferable only when in depth scarring of the deeper buildings is present because otherwise the chance of flap necrosis is increased. For a small skin defect, the trident plasty based on Glicenstein and Hirshowitz represents the therapy of selection. Should an extensive skin defect be discovered after resolving a contracture, one must first examine whether or not or not this can be covered utilizing a free pores and skin graft. Due to the tendency of a skin transplant to shrink, and the practical limitations which thereby develop, the indication for a well vascularised flap may be considered liberally. For dorsal pores and skin defects restricted to the first commissure, the mix of a neighborhood flap with a medium split-thickness pores and skin transplant can, in plenty of circumstances, result in a functional and aesthetically good outcome. In younger kids additional pores and skin transplants to close donor-site defects are incessantly not required donor-site defect. Due to the massive aesthetic donor-site defects, the dorsal thumb transpositional flap according to Spinner ought to solely be used as a third choice. Because of the great significance of the lateral index finger floor for the key grip, the radiolateral index-finger transpositional flap according to Spinner is just employed when no different native flap is on the market. If solely small pores and skin defects are current, the trident plasty according to Glicenstein and Hirshowitz is the first-choice remedy. This is the case when no important constructions like vessels, nerves, tendons or bones are exposed. In the acute state of affairs, coverage of the defect may be performed using a medium split-thickness skin graft. For the reconstruction of secondary skin defects, full-thickness pores and skin grafts ought to be utilized by all means because of the decreased tendency to shrink. The palmar vascular-pedicled transpositional flap based on Vasconez has confirmed itself for the coverage of defects involving the palmar area alone. Because of the risk of secondary retraction, a easy skin transplantation in the area of the commissures should only be carried out in exceptional circumstances. Frequently, the base of the defect has an irregular type, especially when the adductor pollicis muscle and the interosseous palmaris I muscle have been resected. The introduction of Kirschner wires between the metacarpals or as an external fixation delays the beginning of physiotherapy and might result in stiffening in the new position. In the presence of intact pores and skin, the three-flap transpositional plasty in accordance with Schneider and Vaubel is the therapy of first choice. As a second-choice therapy, the butterfly flap in accordance with Shaw and, as a third alternative, the dorsopalmar transpositional flap according to Flatt has proven efficient. To prevent recurrent syndactyly by way of secondary scar formation (web creeping), the indication for added full-thickness pores and skin grafts must be thought-about liberally in the entire three flaps. If the pores and skin in the region of the syndactyly is pathologically altered, the 15 Table 15. In adults, this flap may be considered second choice due to the intensive preparations which are required. Because of the great significance of the lateral index finger floor for the key grip, the radiolateral index finger transpositional flap based on Spinner should only be thought of when no different local flap is on the market. If the skin in the complete area of the dorsum of the hand is pathologically altered as nicely, the native defect protection within the commissural area can only be treated successfully with the palmar vascular-pedicled transpositional flap according to Vasconez. Because of the large useful donor-site defects related to these situations, one other flap should be chosen, especially in handbook employees. In the presence of congenital malformations and polydigital hand accidents in the commissural region, defect coverage by way of the tissue-bank idea according to Chase have to be thought-about, utilizing an unreconstructable index finger (chiroplasty). In men, the distally pedicled posterior interosseous artery flap in accordance with Penteado or Zancolli is the first-choice therapy. Due to the seen dorsal scar on the hand and hair progress in the region of the flap, indications for the utilization of this flap in girls ought to be thought of very fastidiously. Here, the distally pedicled radial artery-fascial flap based on Yang has confirmed suitable. For highly obese patients, all distally pedicled flaps from the region of the forearm have a very thick layer of subcutaneous fatty tissue. In circumstances involving extensive burn injuries and in particular posttraumatic situations, particularly when either native and even distally pedicled flaps from the forearm are unsuitable, pores and skin flap from further distant areas of the body have to be conceived. Due to decreased donor-site defect, the lateral higher arm fascial flap in accordance with Song ought to be preferred over the free microvascular radial artery-fascial flap according to Yang and the free microvascular dorsalis pedis artery-fascial flap in accordance with McCraw and Furlow. In extraordinarily overweight sufferers, a free microvascular fascial flap could be applied and covered with a full- or, no less than, a thick split-thickness pores and skin graft. If free microvascular flaps are contraindicated, distant flaps have to be used for very large defects.
Buy generic asendin 50mg on-lineClinical and histologic responses to gluten withdrawal are necessary in confirming the analysis depression prayer order asendin us. Tropical Pancreatitis Idiopathic continual calcific pancreatitis or tropical pancreatitis is endemic in a quantity of tropical areas including the Indian subcontinent and southern Africa mood disorder due to a general medical condition buy generic asendin from india. Symptoms of recurrent stomach pain typically develop in childhood or adolescence and often persist for eight to 10 years anxiety 10 year old daughter generic 50 mg asendin with mastercard. Exocrine pancreatic insufficiency anxiety forum discount asendin 50 mg online, with a history of passing oil within the stool, finally develops in additional than 25%, and diabetes mellitus develops in more than 50% of affected sufferers. The illness is likely to be genetically determined, and both disease-inducing and disease-protective mutations have been noted. Pancreatic enzymes with a excessive lipase content material often are administered with every meal and are most effective when ingested about halfway via the meal. Therapy of the pain in this illness consists of administration of pancreatic enzymes, celiac plexus block, endoscopic removal of calculi, and surgery with pancreatic drainage (see Chapter 59). Panel C is a Masson trichrome stain showing microsporidia which are much smaller (1 to 2 microns) in diameter. Stool samples are examined by microscopy of moist smears, immediately and after focus (sedimentation and flotation) strategies for ova and cysts, and with special (trichrome and/ or modified acid-fast) stains for coccidian parasites. Hematologic and biochemical analysis is undertaken to establish the presence of particular nutrient deficiencies, together with folate, vitamin B12, and iron. Double-balloon enteroscopy is usually essential to acquire biopsies from areas suspected to be irregular in the jejunum or ileum beyond the attain of standard endoscopes. Rarely, a affected person will require laparoscopy or laparotomy and enteroscopy with full-thickness biopsy to diagnose the small intestinal illness answerable for malabsorption in the tropics. Climatic drivers of diarrheagenic Escherichia coli incidence: a systematic review and meta-analysis. Temperature variability and incidence of diarrhoea in youngsters beneath five-years-old in Cape Town Metropolitan sub-districts. The impact of environmental and climatic variation on the spatiotemporal developments of hospitalized pediatric diarrhea in Ho Chi Minh City. Travel-associated enteric infections recognized after return to the United States, foodborne diseases active surveillance Network (FoodNet), 2004-2009. Prevalence of gastrointestinal pathogens in developed and developing international locations: systematic review and meta-analysis. Enteropathogens and gut irritation in asymptomatic infants and youngsters in several environments in southern India. Prevalence of foodborne pathogens in food from chosen African countries-a metaanalysis. Evidence for public well being dangers of wastewater and excreta administration practices in Southeast Asia: a scoping review. Environmental enteric dysfunction: pathogenesis, diagnosis, and medical penalties. Environmental enteropathy: elusive but important subclinical abnormalities in creating nations. Spectrum of chronic small bowel diarrhea with malabsorption in Indian subcontinent: is the pattern actually changing Spectrum of malabsorption syndrome among adults and elements differentiating celiac disease and tropical malabsorption. A cluster of acute diarrhea suspected to be cholera in French vacationers in Haiti, December 2010. Mapping the burden of cholera in sub-Saharan Africa and implications for control: an analysis of knowledge across geographical scales. Surveillance for travel-related disease-GeoSentinel surveillance system, United States, 19972011. Travel-related acquisition of diarrhoeagenic bacteria, enteral viruses and parasites in a prospective cohort of ninety eight Dutch travellers. Prevalence and characteristics of duodenal villous atrophy in renal transplant sufferers presenting with persistent diarrhea in a developing country. Prevalence of adult celiac disease in India: regional variations and associations. Distinguishing tropical sprue from celiac disease in returning travellers with chronic diarrhoea: a diagnostic problem Guidelines for the investigation of persistent diarrhoea in adults: British Society of Gastroenterology. Tropical sprue: some early investigators favoured an infectious trigger, but was a coccidian protozoan concerned Infectious gastroenteritis as a risk issue for tropical sprue and malabsorption: a case-control study. Seasonal prevalence of overt and subclinical tropical malabsorption in Puerto Rico. Enterotoxigenicity of colonising coliform bacteria in tropical sprue and blind-loop syndrome. Biomarkers of environmental enteropathy, inflammation, stunting, and impaired development in youngsters in Northeast Brazil. Environmental enteropathy: critical implications of a poorly understood condition. Faecal microbiota of healthy adults in south India: comparability of a tribal & a rural inhabitants. Evaluation of the efficacy of oral rehydration solutions using human entire intestine perfusion. Exploring the role of environmental enteropathy in malnutrition, infant improvement and oral vaccine response. Environmental enteropathy, oral vaccine failure and growth faltering in infants in Bangladesh. Tropical enteropathy protects towards Western illnesses in environments of poor sanitation. Implications of acquired environmental enteric dysfunction for progress and stunting in infants and youngsters dwelling in low- and middle-income international locations. Environmental enteropathy is associated with cardiometabolic danger factors in Peruvian kids. Coccidian intestinal parasites among immunocompetent youngsters presenting with diarrhea: are we missing them Diagnostic worth of endoscopy for the prognosis of giardiasis and other intestinal diseases in patients with persistent diarrhea from tropical or subtropical areas. Hymenolepis nana impression amongst children within the highlands of Cusco, Peru: an emerging uncared for parasite an infection. Spectrum of parasitic infections in patients with diarrhoea attending a tertiary care hospital in Western Rajasthan, India. Pathogenesis of tropical sprue: study of antroduodenal manometry, duodenocecal transit time and fat-induced ileal brake. Non�gluten sensitivity�related small bowel villous flattening with increased intraepithelial lymphocytes: not all that flattens is celiac sprue. An electron-microscopic examine of jejunal mucosal morphology in control topics and in sufferers with tropical sprue in southern India. Role of bacterial toxins, bile acids and free fatty acids in colonic water malabsorption in tropical sprue. Duodenal villous morphology assessed utilizing magnification slender band imaging correlates properly with histology in patients with suspected malabsorption syndrome. Responses of small intestinal architecture and function over time to environmental factors in a tropical inhabitants. Burden and aetiology of diarrhoeal disease in infants and young youngsters in devel- 78. Prevalence of microsporidia in healthy individuals and immunocompetent patients with acute and persistent diarrhea. Etiology of diarrhea in youngsters youthful than 5 years attending the Bengo General Hospital in Angola. Intermittent directly observed remedy for stomach tuberculosis: a multicenter randomized managed trial evaluating 6 months versus 9 months of remedy. Immunoproliferative small intestinal disease in south India: a clinical and immunomorphological examine. Clinical symptoms and findings are protean and include weight reduction, diarrhea, malabsorption, fever, arthralgias, pores and skin hyperpigmentation, and dementia. Host immunologic factors are presumed to affect susceptibility to this illness agent.
Asendin 50 mg cheapControl and Prevention Control and prevention require improved housing depression test cesd cheap asendin, use of pesticides and netting mood disorder facts cheap generic asendin canada, and screening of blood for antibody in endemic areas depression definition business discount asendin 50 mg overnight delivery. Entamoeba histolytica�associated diarrheal illness is negatively related to the growth of preschool children: proof from a potential study mood disorder light purchase generic asendin pills. Identification of etiologyspecific diarrhea related to linear development faltering in Bangladeshi infants. A mutation in the leptin receptor is related to Entamoeba histolytica an infection in kids. Leptin signaling in intestinal epithelium mediates resistance to enteric infection by Entamoeba histolytica. Electron microscope studies of experimental Entamoeba histolytica infection in the Guinea pig. Entamoeba histolytica cysteine proteinases disrupt the polymeric construction of colonic mucin and alter its protective perform. Epithelial cell�initiated irritation plays an important function in early tissue injury in amebic infection of human gut. Entamoeba histolytica trophozoites induce an inflammatory cytokine response by cultured human cells by way of the paracrine action of cytolytically released interleukin-1�. A longitudinal study of asymptomatic carriers of pathogenic zymodemes of Entamoeba histolytica. Invadosome-mediated human extracellular matrix degradation by Entamoeba histolytica. Amebiasis and mucosal IgA antibody towards the Entamoeba histolytica adherence lectin in Bangladeshi youngsters. Differential medical features and stool findings in shigellosis and amoebic dysentery. New ideas of amebic liver abscess derived from hepatic imaging, serodiagnosis, and hepatic enzymes in 67 consecutive instances in San Diego. Value of microscopy in the analysis of dysentery related to invasive Entamoeba histolytica. The differentiation of invasive and noninvasive Entamoeba histolytica by isoenzyme electrophoresis. Immunological differentiation of pathogenic and non-pathogenic isolates of Entamoeba histolytica. Pathogenic and nonpathogenic strains of Entamoeba histolytica could be differentiated by monoclonal antibodies to the galactose-specific adherence lectin. Evaluation of an antigen-capture enzyme immunoassay for detection of Entamoeba histolytica in stool samples. Entamoeba gingivalis in human immunodeficiency virus sort 1�infected patients with periodontal disease. Transmission of Entamoeba nuttalli and Trichuris trichiura from nonhuman primates to people. Entamoeba polecki and other intestinal protozoa in Papua New Guinea highland kids. Giardia assemblages a and B in diarrheic patients: a comparative examine in Egyptian youngsters and adults. An outbreak of giardiasis in a nursing house with evidence for multiple modes of transmission. Natural historical past of Giardia an infection of infants and youngsters in rural Guatemala and its influence on physical development. Natural historical past of Giardia lamblia and Cryptosporidium infections in a cohort of Israeli Bedouin infants: a study of a population in transition. A systematic evaluation and meta-analysis of the affiliation between Giardia lamblia and endemic pediatric diarrhea in growing countries. Bacterial, parasitic and viral enteropathogens associated with diarrhoea in Saudi youngsters. Aetiologic brokers of diarrhoeal diseases in hospitalised youngsters in Rawalpindi, Pakistan. Use of multipLex molecular assay for the detection of pathogens in stools from diarrheic sufferers [abstract]. Presented on the 22nd European Congress on clinical microbiology and infectious illnesses. Amebic infections due to the Entamoeba histolytica�Entamoeba dispar complex: a study of the incidence in a distant rural area of Ecuador. Multicenter analysis of the BioFire FilmArray Gastrointestinal Panel for etiologic analysis of infectious gastroenteritis. Association of serum antibodies to adherence lectin with invasive amebiasis and asymptomatic infection with pathogenic Entamoeba histolytica. Treatment of diarrhea attributable to Giardia intestinalis and Entamoeba histolytica or Entamoeba dispar: a randomized, double-blind placebo-controlled study of nitazoxanide. Problems in recognition and prognosis of amebiasis: estimation of the global magnitude of morbidity and mortality. Prevalence of enteric parasites in homosexual patients attending an outpatient clinic. A comparative examine of 4 methods for detecting Giardia lamblia in children with diarrheal illness and malabsorption. Relation in giardiasis to abnormal intestinal structure and function in gastrointestinal immunodeficiency syndromes. Comparison of serum antibody responses to Giardia lamblia of symptomatic and asymptomatic patients. Specific secretory IgA in the milk of Giardia lamblia�infected and uninfected ladies. Role of interleukin-6 in the management of acute and continual Giardia lamblia infections in mice. Interleukin-6-deficient mice are extremely vulnerable to Giardia lamblia an infection however exhibit regular intestinal immunoglobulin A responses in opposition to the parasite. Lactose malabsorption in kids with symptomatic Giardia lamblia an infection: feasibility of yogurt supplementation. Prospective comparison of direct immunofluorescence and standard staining strategies for detection of Giardia and Cryptosporidium spp. Randomized medical research of nitazoxanide in comparability with metronidazole in the treatment of symptomatic giardiasis in youngsters in Northern Peru. In vitro activity of nitazoxanide and associated compounds towards isolates of Giardia intestinalis, Entamoeba histolytica, and Trichomonas vaginalis. Successful treatment of metronidazole- and albendazole-resistant giardiasis with nitazoxanide in a affected person with acquired immunodeficiency syndrome. Dientamoeba fragilis, a protozoan parasite in adult members of a semicommunal group. Vaccination of domestic animals with a novel oral vaccine prevents Giardia infections, alleviates signs of giardiasis and reduces transmission to people. Evidence of an epidemic of Blastocystis hominis infections in preschool youngsters in northern Jordan. Effect of nitazoxanide on morbidity and mortality in Zambian kids with cryptosporidiosis: a randomised controlled trial. A proposed target product profile and developmental Cascade for new cryptosporidiosis remedies. Association of early childhood diarrhea and cryptosporidiosis with impaired bodily fitness and cognitive function four-seven years later in a poor city neighborhood in northeast Brazil. The efficacy of three widespread hospital liquid germicides to inactivate Cryptosporidium parvum oocysts. Effects of Cryptosporidium parvum an infection in Peruvian kids: growth faltering and subsequent catch-up growth. A novel piperazine-based drug lead for cryptosporidiosis from the Medicines for Malaria Venture open access Malaria Box. A high-throughput phenotypic display identifies clofazimine as a potential treatment for cryptosporidiosis. Alga associated with diarrhea in sufferers with acquired immunodeficiency syndrome and in vacationers. Study of Cyclospora cayetanensis in health care amenities, sewage water, and green leafy vegetables in Nepal.
Purchase asendin 50 mg with mastercardThe apparent equivalent and specific nature of the duodenal and proximal jejunal lesion in celiac illness and idiopathic sprue 03 anxiety mp3 buy asendin 50mg on-line. Tissue transglutaminase selectively modifies gliadin peptides which may be recognized by gut-derived T cells in celiac disease depression test accurate cheap asendin 50 mg fast delivery. In vivo antigen problem in celiac disease identifies a single transglutaminase-modified peptide as the dominant -gliadin T-cell epitope mood disorder quizzes asendin 50 mg online. Prevalence of celiac disease in at-risk and not-at-risk groups in the United States: a large multicenter examine depression symptoms checklist buy generic asendin line. The prevalence of celiac disease in Europe: outcomes of a centralized, international mass screening project. Ethnic variations in duodenal villous atrophy in keeping with celiac disease in the United States. Less hidden celiac illness but increased gluten avoidance without a prognosis in the United States: findings from the National well being and diet examination surveys from 2009 to 2014. The coeliac iceberg in Italy: a multicentre antigliadin antibodies screening for coeliac disease in school-age subjects. Immunoglobulins in jejunal mucosa and serum from patients with adult coeliac illness. Gluten, main histocompatibility advanced, and the small intestine: a molecular and immunobiologic method to the spectrum of gluten sensitivity ("celiac sprue"). Slow and incomplete histological and practical recovery in adult gluten-sensitive enteropathy. Predictors of persistent villous atrophy in coeliac disease: a population-based study. In vitro assessment of acetic acid�soluble proteins (glutenin) toxicity in celiac disease. An evaluation of cereals that react with serum antibodies in sufferers with coeliac disease. The gluten response in youngsters with celiac illness is directed toward a number of gliadin and glutenin peptides. Specific nongluten proteins of wheat are novel goal antigens in celiac disease humoral response. In vitro toxicity of gluten peptides in coeliac disease assessed by organ tradition. Safety of including oats to a gluten-free food regimen for patients with celiac disease: systematic review and meta-analysis of scientific and observational research. Serum IgG subclass antibodies to a selection of food antigens in patients with coeliac disease. IgA anti-endomysium antibody: a brand new immunological marker of dermatitis herpetiformis and coeliac illness. Selective deamidation by tissue transglutaminase strongly enhances gliadin-specific T cell reactivity. In vitro cross-linking of gluten into high-molecular-weight polymers with transglutaminase. Immunobiology and immunopathology of human gut mucosa: humoral immunity and intraepithelial lymphocytes. Association between innate response to gliadin and activation of pathogenic T cells in coeliac disease. Interleukin 15: a key to disrupted intraepithelial lymphocyte homeostasis and lymphoma genesis in celiac disease. Report of 10 patients with particular attention to analysis, medical habits, and follow-up. Defective gallbladder emptying and cholecystokinin release in celiac illness: reversal by gluten-free food regimen. Is exocrine pancreatic insufficiency in adult coeliac disease a reason for persisting signs Yield of diagnostic checks for celiac illness in individuals with signs suggestive of irritable bowel syndrome: systematic evaluate and meta-analysis. Factors that enhance danger of celiac disease autoimmunity after a gastrointestinal an infection in youth. Reovirus infection triggers inflammatory responses to dietary antigens and development of celiac disease. Decreased threat of celiac disease in patients with helicobacter pylori colonization. Lower prevalence of celiac disease and gluten-related issues in persons living in Southern vs northern latitudes of the United States. Pregnancy outcome and risk of celiac disease in offspring: a nationwide case-control examine. Antibiotic exposure and the development of coeliac disease: a nationwide case management research. Concordance, illness development, and heritability of coeliac disease in Italian twins. Newly recognized genetic danger variants for celiac illness related to the immune response. Mucosal and systemic IgA anti-gliadin antibody in celiac disease: contrasting patterns of response in serum, saliva, and intestinal secretions. A prospective comparative study of 5 measures of gluten-free diet adherence in adults with coeliac illness. Usefulness of antibodies to deamidated gliadin peptides in celiac disease analysis and follow-up. Serum IgA anti-gliadin antibodies in an grownup inhabitants sample: high prevalence with out celiac illness. Gastroesophageal reflux signs in patients with celiac disease and the effects of a gluten-free diet. Gliadin antibodies identify gluten-sensitive oral ulceration in the absence of villous atrophy. Hyposplenism and gluten-sensitive enteropathy: natural historical past, incidence, and relationship to food regimen and small bowel morphology. Celiac disease and increased danger of pneumococcal an infection: a scientific evaluation and meta-analysis. Risk of fractures in celiac illness patients: a cross-sectional, case-control study. Severe osteopenia in symptom-free adults with a childhood prognosis of coeliac illness. Coeliac illness and the danger of fractures a basic population-based cohort study. Clinical, radiological, neurophysiological, and neuropathological characteristics of gluten ataxia. Interaction between psychiatric and autoimmune problems in coeliac illness patients within the Northeastern United States. The effect of depressive signs on the association between gluten-free food regimen adherence and symptoms in celiac illness: analysis of a patient powered analysis community. Anxiety but not depression decreases in coeliac sufferers after one-year gluten-free food regimen: a longitudinal examine. Increased prevalence of celiac illness in patients with unexplained infertility within the United States. Recurrent spontaneous abortion and intrauterine fetal progress retardation as symptoms of coeliac disease. Anti-tissue transglutaminase antibodies from celiac sufferers are liable for trophoblast injury via apoptosis in vitro. Body mass index and the risk of obesity in coeliac illness treated with the gluten-free diet. Low testosterone in non-responsive coeliac illness: a case series, case-control examine with comparisons to the national well being and diet examination survey. Association between developmental defects of enamel and celiac illness: a meta-analysis. Comparative evaluation of serologic checks for celiac disease: a European initiative towards standardization. Diagnostic testing for celiac disease amongst sufferers with belly symptoms: a systematic evaluate.
|
|