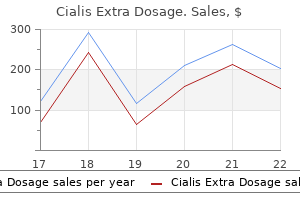
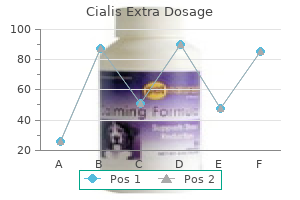
If this is not the case erectile dysfunction in 20s buy cialis extra dosage 40 mg free shipping, then the probabilities will not be properly restricted to the interval [0 erectile dysfunction age onset order cialis extra dosage 60 mg overnight delivery, 1] erectile dysfunction email newsletter order 200mg cialis extra dosage visa. This will be an important consideration in Chapter 8 where we discuss probability density estimation techniques erectile dysfunction ear cheap cialis extra dosage 100mg otc. The cumulative distribution function F (x) is defined as the probability that the random variable X assumes a value less than or equal to a given x impotence at 33 buy cialis extra dosage 200 mg low price. A probability density function impotence klonopin purchase cialis extra dosage 200mg on line, along with its associated cumulative distribution function are illustrated in Figure 2. We let S represent the sample space of an experiment and E represent some event that is a subset of S. Axiom 2 says that an outcome from our experiment must occur, and the probability that the outcome is in the sample space is 1. Axiom 3 enables us to calculate the probability that at least one of the mutually exclusive events E 1, E 2. It is used to define independent events and enables us to revise our degree of belief given that another event has occurred. Conditional probability arises in situations where we need to calculate a probability based on some partial information concerning the experiment. For example, say a couple would like to have two children, and their first child is a boy. The gender of their second child does not depend on the gender of the first child. Thus, the fact that we know they have a boy already does not change the probability that the second child is a boy. Similarly, we can sometimes assume that the value we observe for a random variable is not affected by the observed value of other random variables. If events are independent, then knowing that one event has occurred does not change our degree of belief or the likelihood that the other event occurs. If random variables are independent, then the observed value of one random variable does not affect the observed value of another. Sometimes we can assume independence based on the situation or the experiment, which was the case with our example above. However, to show independence mathematically, we must use the following definition. Later on, we might obtain some additional information about the event that would change our belief about the probability that the event will occur. Suppose our piston rings are purchased from two manufacturers: 60% from manufacturer A and 40% from manufacturer B. Let M A denote the event that a part comes from manufacturer A, and M B represent the event that a piston ring comes from manufacturer B. If we select a part at random from our supply of piston rings, we would assign probabilities to these events as follows: P (M A) = 0. These are our prior probabilities that the piston rings are from the individual manufacturers. Say we are interested in knowing the probability that a piston ring that subsequently failed came from manufacturer A. This would be the posterior probability that it came from manufacturer A, given that the piston ring failed. The additional information we have about the piston ring is that it failed, and we use this to update our degree of belief that it came from manufacturer A. The only way that a piston ring will fail is if: 1) it failed and it came from manufacturer A or 2) it failed and it came from manufacturer B. Applying the Multiplication Rule as before, we have P (F) = P (M A)P (F M A) + P (M B)P (F M B). These are the probabilities that a piston ring will fail given it came from the corresponding manufacturer. They are used to describe distributions, to evaluate the performance of estimators, to obtain test statistics in hypothesis testing, and many other applications. The mean or expected value of a random variable is defined using the probability density (mass) function. If we observe many values of the random variable and take the average of them, we would expect that value to be close to the mean. The mean and variance for continuous random variables are defined similarly, with the summation replaced by an integral. Other expected values that are of interest in statistics are the moments of a random variable. However, a coefficient of skewness equal to zero does not mean that the distribution must be symmetric. Kurtosis measures a different type of departure from normality by indicating the extent of the peak (or the degree of flatness near its center) in a distribution. A ratio greater than 3 indicates more values in the neighborhood of the mean (is more peaked than the normal distribution). If the ratio is less than 3, then it is an indication that the curve is flatter than the normal. Most of these distributions are used in later chapters, so we take this opportunity to define them and to fix our notation. We first cover two important discrete distributions: the binomial and the Poisson. These are followed by several continuous distributions: the uniform, the normal, the exponential, the gamma, the chisquare, the Weibull, the beta and the multivariate normal. Now suppose we repeat this experiment for n trials, where each trial is independent (the outcome from one trial does not influence the outcome of another) and results in a success with probability p. If X denotes the number of successes in these n trials, then X follows the binomial distribution with parameters (n, p). Examples of binomial distributions with different parameters are shown in Figure 2. It is administered to 100 patients, where the outcome for each patient is either cured or not cured. If X is the number of patients cured, then X is a binomial random variable with parameters (100, 0. If we let X represent the number who have a psychiatric disorder, then X takes on values according to the binomial distribution with parameters (50, 0. If the sample contains more than five defective chips, then the process is stopped. If we let X represent the number of people who have a psychiatric disorder, then X is a binomial random variable with parameters (25, 0. We are interested in the probability that at most 3 of the selected people have such a disorder. When n is large and p is small (so np is moderate), then the number of successes occurring can be approximated by the Poisson random variable with parameter = np. The Poisson distribution is also appropriate for some applications where events occur at points in time or space. We see it used in this context in Chapter 12, where we look at modeling spatial point patterns. Some other examples include the arrival of jobs at a business, the arrival of aircraft on a runway, and the breakdown of machines at a manufacturing plant. Let N (t), t 0, represent the number of events that occur in the time interval [0, t]. For each interval [0, t], N (t) is a random variable that can take on values 0, 1, 2. If the following conditions are satisfied, then the counting process { N (t), t 0 } is said to be a Poisson process with mean rate [Ross, 2000]: 1. The number N (t) of events in an interval of length t follows a Poisson distribution with mean t. This means that the distribution of the number of events in an interval depends only on the length of the interval and not on the starting point. Assume that the number of typographical errors per page follows the Poisson distribution with parameter = 0. Note that P (X = 0) + P (X = 1) is the Poisson cumulative distribution function for a = 1 (see Equation 2. What is the probability that at most 3 accidents will occur during the next 2 weeks? One reason is that the uniform (0, 1) distribution is used as the basis for simulating most random variables as we discuss in Chapter 4. This function also plots the normal density, where the area between the specified limits is shaded. Note that as the variance increases, the height of the probability density function at the mean decreases. Note that the default title and axes labels are shown, but these can be changed easily using the title, xlabel, and ylabel functions. You can also obtain tail probabilities by using -Inf as the first element of specs to designate no lower limit or Inf as the second element to indicate no upper limit. Note that it shades the area between the lower and upper limits that are specified as input arguments. This property describes the fact that the remaining lifetime of an object (whose lifetime follows an exponential distribution) does not depend on the amount of time it has already lived. This property is represented by the following equality, where s 0 and t 0: P(X > s + t X > s) = P(X > t). In words, this means that the probability that the object will operate for time s + t, given it has already operated for time s, is simply the probability that it operates for time t. When the exponential is used to represent interarrival times, then the parameter is a rate with units of arrivals per time period. When the exponential is used to model the time until a failure occurs, then is the failure rate. When t is a positive integer, the gamma distribution can be used to model the amount of time one has to wait until t events have occurred, if the interarrival times are exponentially distributed. The mean and variance of a gamma random variable are t E [X] = -, t V (X) = -. The chi-square distribution is used to derive the distribution of the sample variance and is important for goodness-of-fit tests in statistical analysis [Mood, Graybill, and Boes, 1974]. We see that when = t = 1, we have the same probability density function as the exponential with parameter = 1. The mean and variance of a chi-square random variable can be obtained from the gamma distribution. It can be used to model the distribution of the amount of time it takes for objects to fail. For the special case where = 0 and = 1, the Weibull reduces to the exponential with = 1 /. You can also use the function csweibc(x,) to evaluate the cumulative distribution function for a Weibull. The mean and variance of a beta random variable are E [X] = -, + and V (X) = -. It can be used to model a random variable that takes on values over a bounded interval and assumes one of the shapes governed by the parameters.
Amantadine does not interfere with antibody response to influenza vaccination; both may be given together erectile dysfunction drugs after prostate surgery cheap 60 mg cialis extra dosage mastercard. Treatment of influenzal (A2) illness: a modest therapeutic effect (reduction in fever erectile dysfunction by country 200mg cialis extra dosage with visa, congestion erectile dysfunction 19 purchase cialis extra dosage 60 mg fast delivery, cough and quicker recovery) occurs if the drug is given immediately after the symptoms appear erectile dysfunction fertility treatment buy generic cialis extra dosage 60mg on line. Oral bioavailability of rimantadine is higher and it is largely metabolized by hydroxylation followed by glucuronide conjugation erectile dysfunction treatment pdf cheap cialis extra dosage 60 mg with amex. Dose and clinical application in influenza A is similar to amantadine and it is being preferred over the latter erectile dysfunction causes divorce cialis extra dosage 60mg on line. Oseltamivir this newer anti-influenza virus drug is a sialic acid analogue with broad spectrum activity covering influenza A (amantadine sensitive as well as resistant), H5N1 (bird flu), nH1N1 (swine flu) strains and influenza B. It is an ester prodrug that is rapidly and nearly completely hydrolysed during absorption in intestine and by liver to the active form oseltamivir carboxylate with an oral bioavailability of ~ 80%. It acts by inhibiting influenza virus neuraminidase enzyme which is needed for release of progeny virions from the infected cell. In many areas oseltamivir-resistant H1N1 (seasonal influenza) and H5N1 have been encountered, though swine flu (nH1N1) is still mostly sensitive. Some oseltamivir-resistant strains remain susceptible to zanamivir and vice versa. Oseltamivir is indicated both for prophylaxis as well as treatment of influenza A, swine flu, bird flu and influenza B. Started at the onset of symptoms, it is the most effective drug; reduces the severity, duration and complications of the illness. Zanamivir Another influenza A (including amantadine-resistant, nH1N1, H5N1 strains) and influenza B virus neuraminidase inhibitor that is administered by inhalation as a powder due to very low oral bioavailability. The mechanism of action, clinical utility and efficacy of zanamivir are similar to that of oseltamivir. Some variant strains resistant to oseltamivir remain sensitive to zanamivir and vice versa. It can be used as an alternative to oseltamivir, and is equally effective in reducing severity, duration and complications of the disease. Esterases in the intestine and liver release the active drug during absorption to attain oral bioavailability of ~60% in terms of adefovir, which is then distributed in whole body water. Clinical, biochemical (liver function tests), histological, serological and virological response occurs in nearly 50% patients within 1 year. Side effects are sore throat, headache, weakness, abdominal pain and flu syndrome. Nephrotoxicity occurs at higher doses and in those with preexisting renal insufficiency. Due to very low oral absorption, it is used as the disoproxil ester prodrug, which not only improves bioavailability, but also intracellular passage of the active form. Remarkably, renal toxicity is quite rare, though slight increase in serum creatinine occurs. In a comparative study, higher percentage of patients responded within one year of use than with adefovir. Tenofovir-resistance has not developed during treatment of chronic hepatitis B, and it is effective in lamivudine-resistant cases. They have nonspecific antiviral as well as other complex effects on immunity and cell proliferation. Interferons bind to specific cell surface receptors and affect viral replication at multiple steps, viz. It is degraded mainly in liver and kidney, and remains detectable in plasma for 24 hours. Complexed with polyethylene glycol (peginterferon), it is absorbed more slowly- exerts more sustained effects, permiting weekly administration and improving clinical efficacy. Nebulized ribavirin is used for respiratory syncytial virus bronchiolitis in infants and children, particularly those with congenital heart disease, prematurity or other high risk conditions. Combination with oral ribavirin increases number of responders, and decreases chances of relapse. Condyloma acuminata: caused by papilloma virus is usually treated with topical podophyllin. Interferons are also used in chronic myeloid leukaemia, follicular lymphoma, cutaneous T-cell lymphoma and multiple myeloma. Recently few drugs for the newer targets have also become available for use in patients who have failed several regimens employing the 3 major groups of drugs, and have viral multiplication despite optimized background therapy. Finally, viral particles are assembled and matured after fractionation of the polyprotein by viral protease. The major dose-related toxicity is peripheral (stocking and glove) neuropathy, which may be irreversible, and rarely acute pancreatitis. Nausea, anorexia, abdominal pain, headache, insomnia and myalgia are common at the start of therapy, but diminish later. Myopathy, pigmentation of nails, lactic acidosis, hepatomegaly, convulsions and encephalopathy are infrequent. Stavudine and zidovudine exhibit mutual antagonism by competing for the same activation pathway. However, beneficial effects are limited from a few months to a couple of years after which progressively non-responsiveness develops. It should also not be combined with didanosine, because both cause peripheral neuropathy. Frequent peripheral neuropathy, lipodystrophy, lactic acidosis, and rarely pancreatitis are the serious adverse effects which have restricted its use. However, certain lamivudine-resistant mutants become slow growing and have lower virulence. Abacavir should never be given again to a patient who has developed this reaction. Side effects are few- headache, fatigue, rashes nausea, anorexia, abdominal pain. Tenofovir was initially used only in previously treated patients, but because of good tolerability profile, it is now being included in first line regimens as well. Tenofovir containing regimens have been found at least as effective and less toxic as other first line regimens. Their locus of action on the enzyme is also different, and they are non-competitive inhibitors. Nevirapine is started at a lower dose (200 mg/day); the dose is doubled after 2 weeks when its blood levels go down due to autoinduction. The polyprotein is broken into various functional components by this protease enzyme. Because they act at a late step of viral cycle, they are effective in both newly as well as chronically infected cells. Of particular concern are lipodystrophy (abdominal obesity, buffalo hump with wasting of limbs and face), dyslipidaemia (raised triglycerides and cholesterol) which may necessitate hypolipidaemic drugs, and insulin resistance. Drug interactions, nausea, diarrhoea, paresthesias, fatigue and lipid abnormalities are prominent. Raltegravir is an orally active drug that blocks this step by inhibiting the integrase enzyme. Fusion of the two membrances is thus prevented and entry of the virus into the cell is blocked. Attachment of the virus and subsequent entry of viral genome into the cell is thus interfered. Though a number of side effects are reported, tolerability in general is satisfactory. Since it blocks one of the human chemokine receptor, there is concern about impaired immune surveillance and increased risk of infection/malignancy. Greater the suppression of viral replication, lesser is the chance of emergence of drug resistant virus. Various professional bodies and health authorities have framed treatment guidelines from time-to-time. Addition of a fourth drug affords no additional benefit; may be tried in failed patients only. Due to availability of multiple drugs, a variety of combination regimens are possible and have been employed. However, no specific combination can be considered optimal initial regimen for all patients. Tenofovir is included when there is toxicity or other contraindication to both zidovudine and stavudine 3. They are more convenient with lower pill burden, simpler dosing schedules, more acceptable, better tolerated and produce less metabolic complications. If drug toxicity develops, either the entire regimen should be interrupted or the offending drug should be changed. Drugs considered relatively safe during pregnancy are: zidovudine, lamivudine, nevirapine, nelfinavir, saquinavir. With repeated failures it may become more difficult to construct an active combination. Therapy should not be discontinued during an acute opportunistic infection, except in case of intolerance, interactions or toxicity. Failure is due to development of resistance to one or more components of the regimen. Treatment failures are to be anticipated and occur invariably after one to few years. The failed regimen should be changed entirely (all 3 drugs changed) to drugs that have not been administered earlier. In designing second line regimens, drugs with known overlapping viral resistance should be avoided. If the drugs received by the source person is known, prophylactic regimen may be individualized to include at least 2 drugs that the source has not received. The likelihood of preventing infection declines with the delay; some guidelines do not recommend starting it beyond 72 hours of exposure. Malaria, caused by 4 species of the protozoal parasite Plasmodium, is endemic in most parts of India and other tropical countries. However, due to the development of insecticide resistance among mosquitoes and other factors, it staged a comeback in the mid 1970s (6. The bark of Cinchona tree, growing in Peru, was introduced in Europe in the early 17th century as a cure for fevers. Due to enormous military importance of malaria and its treatment, intense activity was initiated for the development of antimalarial drugs. Proguanil was introduced in 1945 by the British as a well tolerated clinical curative. None of the above drugs were found to be capable of preventing relapses in vivax malaria. Pyrimethamine was produced in 1951 under a planned post-war research programme for antimalarial drugs. However, the most significant advance is the Chinese herb derived fast acting Artemisinin compounds, the latest one of which is a synthetic derivative Arterolane developed in India. Stages and forms of the parasite at which different types of antimalarial drugs act are indicated. Lumefantrine Fastest Short *Do not kill gametes but may inhibit their development in mosquito. Antimalarials that act on erythrocytic schizogony are called erythrocytic schizontocides, those that act on preerythrocytic as well as exoerythrocytic (P. Antimalarial drugs exhibit considerable stage selectivity of action (see Table 59-1). Causal prophylaxis the preerythrocytic phase (in liver), which is the cause of malarial infection and clinical attacks, is the target for this purpose. A combined formulation of atovaquone (250 mg) + proguanil (100 mg) is commonly used as a prophylactic by Americans and other western travellers visiting malaria endemic areas. Suppressive prophylaxis the schizontocides which suppress the erythrocytic phase and thus attacks of malarial fever can be used as prophylactics. Though the exoerythrocytic phase in case of vivax and other relapsing malarias continues, clinical disease does not appear.
In the case of supplementation erectile dysfunction vs impotence discount cialis extra dosage 40 mg free shipping, the additional costs may include the time and logistics costs of the distribution of the supplement (which are not always reported) erectile dysfunction at age 30 purchase 60mg cialis extra dosage with visa, and again impotence 16 year old discount cialis extra dosage 50 mg without prescription, the costs associated with monitoring and evaluation erectile dysfunction recovery time discount 60mg cialis extra dosage mastercard. Typical costs incurred by a wheat flour fortification programme (with iron and zinc) are set out in Table 9 impotence over 40 cheap 40mg cialis extra dosage fast delivery. The estimated unit costs of various past supplementation and fortification programmes ved erectile dysfunction treatment 100mg cialis extra dosage with visa, compiled by Levin et al. According to these data, unit costs for supplementation are consistently higher than those for fortification. The cost differential is largely dependent on what proportion the target population is of the whole population; fortification becomes increasingly cost-effective the higher the proportion of the population in need of the intervention. However, for iron the situation is reversed: per person iron supplementation is at least 10 times more costly than fortification but the prevalence of anaemia is well over 10% in most developing country populations. In this case then, mass fortification would most likely be the more cost-effective strategy. It should be stressed that these conclusions are based on average data and cannot be applied to all settings; the relative costeffectiveness of supplementation and fortification will vary markedly across countries according to both the unit cost of the intervention and the fraction of population targeted. Another factor to consider in the supplementation versus fortification debate is the effectiveness of the intervention itself; this can be highly variable. In the case of vitamin A deficiencies, both supplementation and fortification have been shown to be effective in impact evaluations (33,46). In areas of endemic iodine deficiency, salt iodization programmes have also been shown to be highly effective (25,359). However, the evidence for the effectiveness of iron interventions is less clear cut (see section 1. An additional 50% of the cost of quality assurance and monitoring training was included to cover the zinc assessment. The cost per year has therefore been adjusted to take account of these differences in the duration of protection provided by the intervention. On the other hand, despite the fact that iron supplementation has proved to be efficacious in controlled trials (360), many iron supplementation programmes have been relatively ineffective in improving anaemia status, even in targeted subgroups. One possible explanation for this is apparent discrepancy is that in many cases iron deficiency is not the main cause of the observed anaemia, but rather it is some other factor. However, in terms of the magnitude of the calculated costeffectiveness, different outcome measures do not always yield the same result. The most useful outcome or effect measures for cost-effectiveness analyses tend to be those which also provide information on the causes of the change in nutritional status. This is particularly helpful when making comparisons with other studies, which may have employed a different outcome measure. If restricted to using only a single outcome measure, then it is desirable to select the one that can be linked to other outcomes of interest. In the iron example above, the proportion of the population removed from anaemia is the most useful effect indicator, because it is possible to link anaemia status. Despite the inherent variability in the cost-effectiveness of food fortification interventions, it is not necessary to perform analyses for all programmes and for all conditions. Nevertheless, information should be obtained for a selection of programmes operating under a range of conditions. The effects of food fortification, for example, improved productivity in women, will only partially show up as market benefits. Fortification may well result in important nonmarket benefits, such as better child-care, which will affect the market productivity of the next generation. Ideally then, non-market benefits should be valued, by using shadow prices or contingent valuation methods. Nevertheless, even this low rate of discount still favours interventions with immediate benefits. The alternative is a prevalence study, in which costs of fortification are compared with the existing costs attributable to deficiency. The latter requires fewer assumptions, is simpler to undertake, and may be quite useful for advocacy purposes (see Chapter 10). The sample calculations require several key assumptions to be made concerning the economic consequences of deficiency (Table 9. Assumptions must also be made about the effectiveness of a given fortification programme. Productivity loss associated with anaemia is 5% (light manual work), 17% (heavy manual work) and 4% in all other kinds of work. Under such circumstances, it is instructive to conduct a sensitivity analysis, according to the key assumptions made. This involves repeating the calculations several times, varying each of the key parameters in turn. Although there are subsequent productivity effects, the more immediate benefit of vitamin A supplementation in children is a reduction in child morbidity and mortality. This represents the cost of providing 100% of the daily requirements of vitamin A for the population in wheat flour, or 75% of the daily requirements of preschoolaged children via margarine (O. The costs per death averted for the latter are typically significantly higher, which suggests that vitamin A fortification would be a very cost-effective intervention for reducing childhood mortality in country P. Although in many respects urinary iodine excretion is a better indicator of iodine deficiency (it tracks improvements in iodine intake more rapidly (6), at present, such data are not widely available for many countries. Nor is the relationship between urinary iodine excretion and birth outcomes well documented, although it is anticipated that this will become clearer in the future. These calculations make the critical assumption that iodine fortification programmes are 100% effective, i. However, it is generally accepted that only about half of the cases of anaemia are in fact iron-deficiency anaemia; conversely, there are a considerable number of iron deficiency cases that are not associated with anaemia (see section 3. Despite its being an imperfect indicator of iron deficiency, anaemia is nevertheless used in this analysis in the absence of alternative inexpensive and easy-to-apply tests of iron deficiency (see discussion in Ross & Horton (365). Although the prevalence of anaemia (Preanemia) is not necessarily congruent with presence of iron deficiency, it is nevertheless an appropriate indicator to use here since the estimates of productivity losses employed (see Table 9. If in country P, the proportion of employment in agriculture is 25%, the overall prevalence of anaemia in the population is 37. However, the study was limited to children aged 7, 11 and 15 years, and was based on a before-andafter comparison, rather than on an intervention/control design. If it is assumed that in country P the same absolute decrease in anaemia prevalence can be obtained as was achieved in Venezuela (for the whole population, not only children), then the proportional reduction in anaemia due to the fortification programme would be: 0. Additional benefits for both iodine and iron, not taken into account here, include improvements in cognitive development and in school performance in children. In turn, a 10 g/l improvement in haemoglobin levels is associated with an odds ratio of 0. Analyses of cost-effectiveness are particularly useful for comparing different interventions that share the same outcome. Although the latter measure combines mortality and morbidity outcomes into a single indicator, its calculation is generally more demanding in terms of data needs and assumptions. Food fortification with vitamin A is highly cost-effective in reducing mortality in children, as is supplementation with iron in pregnant women. Fortification becomes increasingly cost-effective the higher the proportion of the population in need of the intervention. Fulfilment of these objectives not only requires political commitment and corporate support, but also that national laws and regulations, manufacturing and marketing practices, and community norms, policies and structures be strengthened or modified in some way so as to bring adequately fortified foods to those who need them most. Furthermore, individuals are likely to need guidance and encouragement before they willingly incorporate fortified products into their diets, modify their dietary practices that affect the absorption of nutrients in foods, and adopt household storage and cooking techniques that maximize the nutrient value of the foods they eat. To increase its chances of success, a fortification programme needs to be supported by a range of well-coordinated communication activities that promote individual, community, corporate and political change. In this respect it is important to be aware that messages about the benefits of fortification can be communicated in a number of different ways, using a variety of techniques, to very different effect depending on the intended audience. By outlining some of the options available, the main purpose of this chapter is, therefore, to help micronutrient programme managers understand the different communication needs of various sectors and so direct their communication activities more efficiently. Experience has shown some approaches to be particularly useful for encouraging individuals to adopt healthier behaviours. In practice, however, it is not simply a question of choosing one approach over another, but finding the right blend of strategies and tactics that together achieve programme objectives (367). A useful framework for analysing communication needs, in which education, marketing and legislation are viewed as interconnected approaches to managing social and health issues, has been suggested by Rothschild (373). By describing the relationship between various activities in terms of individual decision-making and perceived costs and benefits (Figure 10. The crafting and delivery of messages and strategies, based on consumer research, to promote the health of individuals and communities (V. The process actively involves the target population, who voluntarily exchange their time and attention for help in meeting their health needs as they perceive them" (370). Persuading others to support an issue of concern to an individual, group or community. May involve, "the strategic use of the mass media as a resource to advance a social or public policy initiative" (371). A broad scale movement to engage large numbers of people in action for achieving a specific development goal through self-reliant effort. Social mobilization is most effective when it is composed of a mix of advocacy, community participation, partnerships and capacity-building activities that together create an enabling environment for sustained action and behaviour change (372). This approach is most effective when the benefits of a change are obvious, and the change does not appear costly to the person or group being asked to make the change. It had been assumed in the past that only a minimal amount of communication was needed to "educate" the public, opinion leaders in the scientific community and industry about the benefits of adding nutrients to foods. However, experience with salt iodization has demonstrated that in reality a far more negotiated approach is required. However, at the individual level this need is largely unrecognized because people neither crave micronutrients nor realize that they are deficient. Since raw data on the prevalence of deficiency are often difficult for the general public to understand, by themselves they do not suffice for providing individuals with a believable rationale for changing their shopping, food preparation or dietary habits. What is needed instead is a more user-friendly message, preferably one that is tailored to suit the information needs and cognitive ability of the recipients (see Box 10. Whenever technical experts disagree, the public tends to ignore all scientific evidence until such time 226 10. Information for the purpose of providing knowledge must be simple, clear and unambiguous. For fortification programme managers it can sometimes be difficult to achieve a consensus between competing claims of effectiveness, safety, quality and cost of a given intervention. For instance, whereas public health professionals tend to advocate the most appropriate fortificant levels for maximum impact, or recommend use of those fortificant compounds that offer the highest bioavailability, producers will try to minimize changes in product quality and cost. Hence, at the outset of food fortification programmes, it is important to attempt to integrate and translate the technical language and jargon of the public health, food science and business sectors into a common vocabulary that all the various professionals involved can understand. Technical language and jargon should be reserved for professional communications; the public will require a more carefully crafted approach altogether, and one that is based on the appearance of scientific consensus in order to achieve maximum penetration. In the context of health, most laws and regulations are aimed at achieving the collective good over individual desires or profit. For maximum impact, advocacy should be: - focused on one or a very limited number of issues; - get to the point quickly and end quickly; - add emotional content and localization; - answer the question: Why should we care? When any concerned group organizes to change a law or policy, their primary tool is advocacy.
Because of their high fat content erectile dysfunction pump infomercial buy 200mg cialis extra dosage with amex, nuts contain 140 more calories per ounce than grains and legumes impotence symptoms order cialis extra dosage 50 mg amex. On the other hand generic erectile dysfunction drugs online cialis extra dosage 100mg visa, the fat in unroasted nuts is unsaturated and unprocessed erectile dysfunction natural foods generic 60mg cialis extra dosage with visa, an advantage over vegetable shortening or animal fat erectile dysfunction treatment with fruits proven 40mg cialis extra dosage, which are saturated fats impotence remedy order 100 mg cialis extra dosage fast delivery. Brazil nuts, hazelnuts, hickory nuts, peanuts, pecans, pistachios, and walnuts provide 4. Americans who eat nuts frequently seem to have a lower risk of heart attack and coronary disease. Snack nuts (roasted nuts) are usually roasted in palm kernel oil or coconut oil, increasing their saturated fat content. A cup of roasted peanuts contains 1,000 mg of sodium, one-third of the suggested daily intake. If unsweetened and if no additives are used, nut butters are equivalent to a typical nut snack. Although usually eaten as a snack food, chopped nuts can be added to fruit salads, yogurt, pancakes, pilaf, and baked goods for a pleasing variety. Chestnuts differ from other nuts in that they contain three to four times more carbohydrate and less fat and protein than other nuts, and their overall nutrient profile resembles that of dry corn or rice products. In general, shelled nuts are sold vacuum-packed to increase their shelf life; they should be refrigerated or frozen to slow rancidity due to their high unsaturated oil content. Peanuts contain 26 percent protein, the highest protein content among commonly available nuts. Defatted nut meal such as almond meal and peanut flour is used as a protein-rich flour. Mixtures of grains and cereals with nuts provide a complementary mixture of essential amino acids that more nearly matches dietary requirements than either alone. Typically, nuts contain up to seven times the amounts of these minerals as found in other unprocessed foods. Vegetables, fruits, nuts, legumes, spices, and teas contain substances that possibly help prevent many of the chronic, degenerative diseases that characterize aging in populations of developed nations. In terms of anticancer effects, the various chemicals in foods could affect the two stages of development of cancer. These agents may block the activation of carcinogens, stimulate the levels of protective enzymes that detoxify carcinogens, or trap carcinogens. They are strong antioxidants, linked with cancer prevention, increased immunity, and lowered risk of cardiovascular disease. Regardless of the source, food-derived preparations need to be standardized (that is, the identities and levels of key active ingredients should be known). Many ingredients in foods, particularly those derived from plants, possess the ability to nutrient An ingredient of foods that can be used by the body for growth and maintenance of health. Foods are mixtures of nutrients, and the relative 466 nutrient density amounts of the various nutrients in a given food depend on conditions of growth, storage, degree of processing, and method of cooking. Certain nutrients must be supplied by the diet because the body cannot manufacture them. More than 50 different kinds of nutrients have been identified; 40 are definitely required for human growth, development, and health. These nutrients are used for energy, to supply building blocks to replace worn out cell constituents, and for normal cell and tissue function. The body represents about 65 percent water; weight-wise, the diet must supply more water than any other nutrient. Requirements A majority of essential nutrients are sufficiently well characterized to warrant recommendations for daily allowances, whatever their source. Nutrient recommendations rely upon biochemical research, clinical case histories of nutrient-deficient individuals, human experimentation with suboptimal diets, animal growth experiments and examination of nutrient intake of healthy people. Reliance on foods containing high levels of fat or calories-as sweets, fatty snack foods, and many highly processed foods-crowds out micronutrients like vitamins and trace minerals. The higher the nutrient density, the closer the food is to the initial unprocessed food and the more key nutrients it has. Excessive calories contribute significantly to the problem of overweight facing many Americans. Thus a food can be considered nutritionally equivalent if it is not nutritionally inferior. A food that provides fewer fat calories but equal levels of essential nutrients can be regarded as nutritionally superior. Digestibility, nutrient uptake and interrelationships among nutrients influence nutrient availability in fabricated foods. An elderly patient may not be able to purchase or prepare adequate food because of physical limitations. Nutritional assessment entails a comprehensive health evaluation: Medical history, diet analysis, physical exam, and measurement of height and weight can reflect nutrient status. Most nutrition programs require training in food science and the biological sciences. A graduate of a program in nutrition, nutrition education, or dietetics is likely to be qualified. A number of professional organizations offer certification programs that assure high standards and are open to qualified health care professionals, such as the International and American Associations of Clinical Nutritionists and the Certification Board of Nutrition Specialists. There are six species, including common oats and cultivated red oats, that are grown in the Americas. Oats are classified as winter and spring varieties, according to their planting time. An inedible, loose, pithy hull surrounds the kernel, or groat, and must be removed for human consumption. Oat flakes, prepared by steaming and flaking whole kernels, are the basis for porridge. Oat bran has been used as a fat substitute to reduce fat in beef and pork sausage products. This fat substitute is used in baked goods and processed meats, and other products are under development. Oatmeal Hot oatmeal is a traditional breakfast, and its emergence as an important source of fiber has caused a resurgence in popularity. However, processed, cold oat breakfast cereals contain much less fiber (about 2 g per serving). Dry oatmeal contains about 14 percent protein, but cooked oatmeal is only about 2 percent protein. Nutrient content of regular cooked oatmeal or rolled oats, (1 cup fortified) is: 145 calories; protein, 6 g; carbohydrate, 25. In 1998 the federal government adopted new standards for determining whether a person is overweight or obese. Before then, people were considered overweight if their weight was at least 10 percent to 20 percent over optimal body weight. Obesity was defined as being more than 25 percent over the optimal body weight for 468 obesity 469 men and 30 percent over the optimal body weight for women. According to statistics compiled by the World Health Organization, obesity is increasing worldwide-an estimated 1. The conditions were already responsible for as many as 300,000 premature deaths each year, costing the nation an estimated $117 billion. Childhood obesity has increased dramatically since 1965 in the United States, reflecting an increased prevalence of obesity among children in Western countries. The rising rate of overweight and obesity among young people is of special concern because childhood and adolescence is often a time in life when people are the most active and therefore least likely to gain excessive weight. Also, unhealthy nutrition and lifestyle habits that lead to overweight and obesity developed during this time have a good chance of continuing into adulthood. The number of obese Americans has increased, despite a national preoccupation with dieting. Being obese or overweight often brings a profound social stigma affecting personal life, life insurance premiums, and employment opportunities. Nevertheless, in the 1980s the renewed interest in healthy lifestyles in America apparently affected a limited number of people. Types of Obesity Hyperblastic obesity is characterized by an excessive number of fat cells. Increased fat cell size is classified as hypertrophic obesity, and individuals with hyperblastic-hypertrophic obesity have increased numbers of enlarged fat cells in their adipose tissue. Hyperblastic obesity is usually associated with childhood, while hypertrophic obesity develops later in life and is associated with diabetes and other aspects of metabolic imbalance. For persons who are 40 pounds overweight, the death rate is estimated to be 80 percent higher during the next 25 years of their life. One clue to understanding the relationship between obesity and elevated blood fat is the observation that obese people have higher insulin levels, which seems to promote higher blood lipids. Male-patterned obesity, with fat deposited primarily in the abdomen and trunk, is called android obesity (the "spare tire" or "apple" profile). Abdominal fat may be more readily converted to cholesterol than fat deposited elsewhere. Pear-shaped people, with fat accumulation around the hips, do not experience as much diabetes or high blood pressure or as many heart attacks as those whose fat is around the middle. The hypothalamus plays a critical role in eating and balancing energy requirements with intake. The lateral hypothalamus controls eating activity; the paraventricular nucleus regulates nutrient balance and the ventromedial hypothalamus regulates energy balance by regulating the sympathetic nervous system, which helps the body adapt to stress. Obesity is linked to altered function of the brain stem and hypothalamus and to changes in the autonomic nervous system, which regulates energy expenditure and regulates thermogenesis. Several hypotheses link food intake and energy balance to regulate body weight through an interplay between the endocrine system and the nervous system. A hypothetical very general control system involves the following components: A proposed "controller" resides in the brain. Signals leaving the brain regulate heat production, physical activity, food intake, energy storage as fat, and metabolism for doing work and producing heat. Nutrients and hormones from various glands and fat cells are then carried back to brain centers that in turn generate signals that are interpreted by the hypothalamus to diminish eating. In 2002 researchers reported that the recently discovered "hunger hormone" ghrelin might be a significant factor in determining why some people become obese and why most people find it hard to keep weight off once it is lost. A study of a small group of obese people revealed they had much higher blood levels of ghrelin, which is produced by stomach cells, after they lost weight through diet control and exercise. In contrast, people who lost weight after gastric bypass surgery, which reroutes the flow of food, had low levels of ghrelin. The extremely low levels of ghrelin in people who had undergone gastric bypass surgery might explain why these people were usually more successful in keeping weight off. Researchers cautioned that the results were preliminary and that ghrelin is probably only one of many tools the body uses to regulate body weight. Another hypothesis predicts a "set point" that tends to keep body weight at a constant level. According to the "set point" hypothesis for body weight, each person has a biologically determined body weight, believed to be inherited. Thus, an obese person with large numbers of fat cells could crave food, leading to excessive eating after dieting. According to a related hypothesis, some obese people earlier in their lives, perhaps during early childhood, ate much more than their bodies needed during their formative years. According to this proposal, this event patterned the body for burning energy and storing fat. Once overweight, obesity in these individuals could be sustained even when consuming an average amount of food. Recent discoveries shed light on the relationships among obesity, satiety, and noninsulin dependent diabetes. Leptin signals the brain to reduce consumption of fatty foods and possibly to increase the basal metabolism of fat cells. Therefore, leptin helps regulate body weight by limiting body fat accumula- obesity 471 tion. Researchers now believe obese people often make more than enough leptin, but the brain does not respond effectively to shut down eating because its binding sites or cell signaling mechanisms are defective. Specifically, the region known as ventromedial nucleus, which regulates satiety, may be involved. Leptin could shut off signals in the brain that direct feeding (hunger signals), including neuropeptides. One possibility is neuropeptide Y, which induces lab animals to eat more carbohydrate and fat. In the set point model, leptin could act like a thermometer: When the body gets too thin, less leptin is made, more food is eaten, and less energy is consumed. When the body gets too fat, more leptin is made, less food is consumed, and more energy is burned. Under normal conditions norepinephrine produced by the sympathetic nervous system stimulates fat cells to burn stored fats. The implication is that with a faulty neurotransmitter attachment site in fat tissue, the body burns less fat efficiently and calories accumulate. As an alternative to the set point hypothesis, the "settling point" theory proposes that body weight is not fixed, but that it is maintained according to feedback loops that are determined by an interplay between genes and environment. Systems controlling hunger and satiety respond rapidly to dietary protein and carbohydrate, but the feedback from a fatty meal may be too slow to prevent overconsumption. Fat cells are added during childhood and it could very well be that how much fatty food is consumed and how many calories are burned before adulthood has a major impact for the risk of obesity. Inheritance as well as diet and medical history can contribute to excessive weight gain and many questions about the detailed interrelationships remain unanswered.
Buy discount cialis extra dosage 50mg. Erectile Dysfunction: Harbinger of Heart Disease?.
References
Hofbauer, C., Anderson, P.V., Juul, P. et al. Late mesh rejection as a complication to transabdominal preperitoneal laparoscopic hernia repair. Surg Endosc 1998;12: 1164-1165.
Glenville M, et al. Effects of sleep deprivation on short duration performance measures compared to the Wilkinson auditory vigilance task. Sleep 1978;1(2): 169-76.
Rozich JD, Carabello BA, Usher BW, et al: Mitral valve replacement with and without chordal preservation in patients with chronic mitral regurgitation. Mechanisms for differences in postoperative ejection performance, Circulation 86:1718-1726, 1992.
Atiq-ur-Rehman M, Naseem A, Hussain T. Comparison of diagnostic yield of AFB with sputum induction to spontaneous sputumexamination in suspected pulmonary tuberculosis. J CollPhysicians SurgPak 2009; 19: 506-509.
Jackson CE, Barohn RJ, Mendell JR. Acute paralytic syndrome in three American men. Arch Neurol. 1993;50:732-735.